
licensee can be completed effortlessly. Just use FormsPal PDF editing tool to complete the task quickly. Our editor is continually evolving to deliver the very best user experience attainable, and that's due to our resolve for constant enhancement and listening closely to customer feedback. This is what you would want to do to start:
Step 1: First of all, access the tool by clicking the "Get Form Button" above on this site.
Step 2: Using this state-of-the-art PDF editing tool, you're able to do more than simply complete blanks. Try all of the functions and make your docs appear great with custom text put in, or fine-tune the file's original input to excellence - all that comes with the capability to insert your personal pictures and sign the file off.
Completing this form generally requires care for details. Ensure that every single blank field is filled out properly.
1. Fill out your licensee with a number of essential fields. Gather all the necessary information and ensure nothing is omitted!
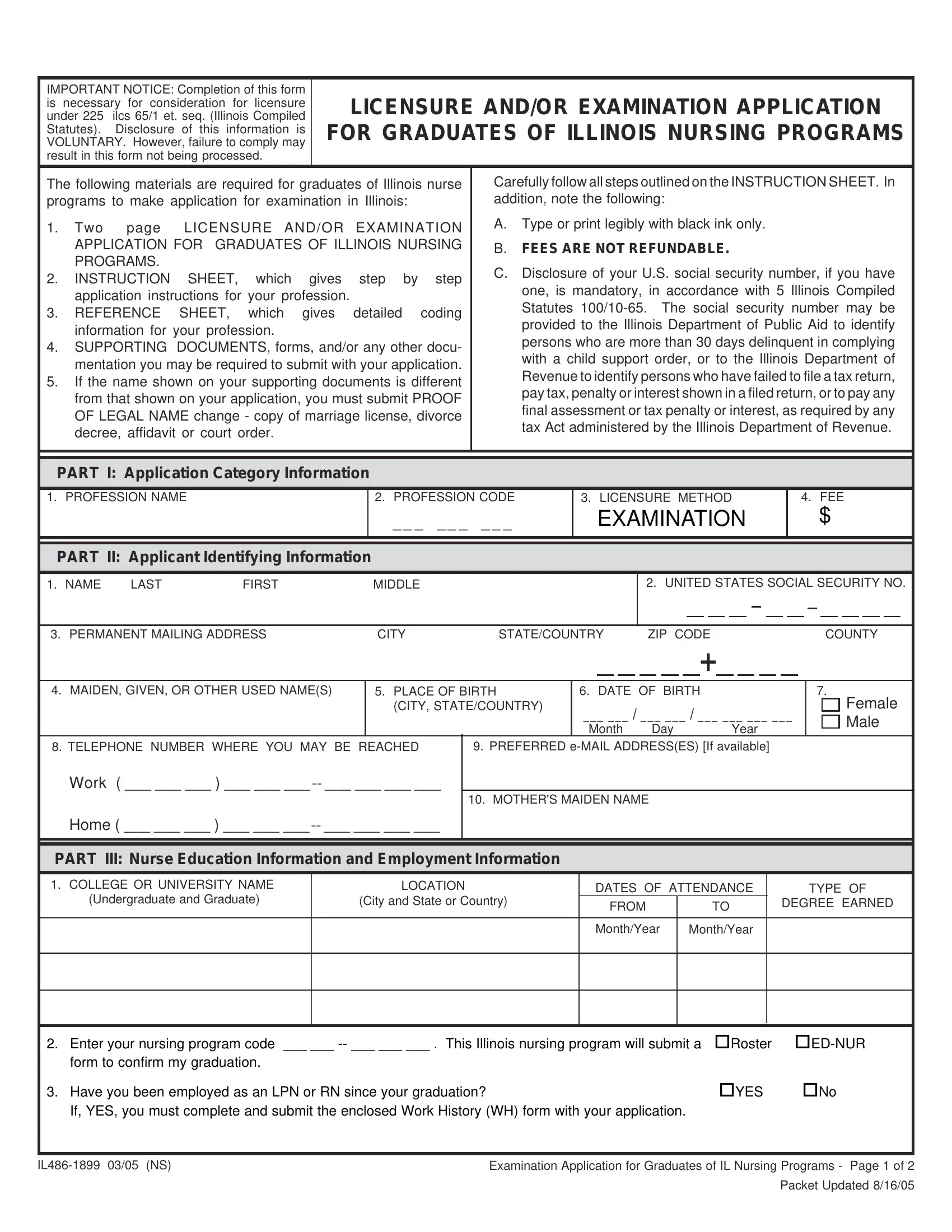
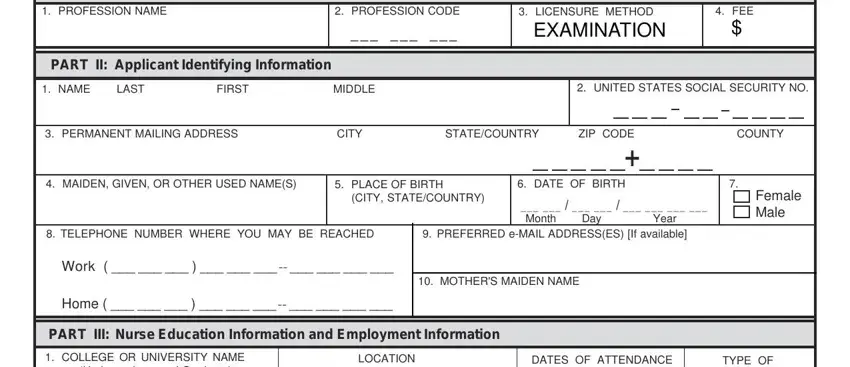
2. Just after performing the last section, go to the next part and fill in the necessary details in these blank fields - PROFESSION NAME, PART II Applicant Identifying, PROFESSION CODE, LICENSURE METHOD, EXAMINATION, FEE, NAME, LAST, FIRST, MIDDLE, UNITED STATES SOCIAL SECURITY NO, PERMANENT MAILING ADDRESS, CITY, STATECOUNTRY, and ZIP CODE.
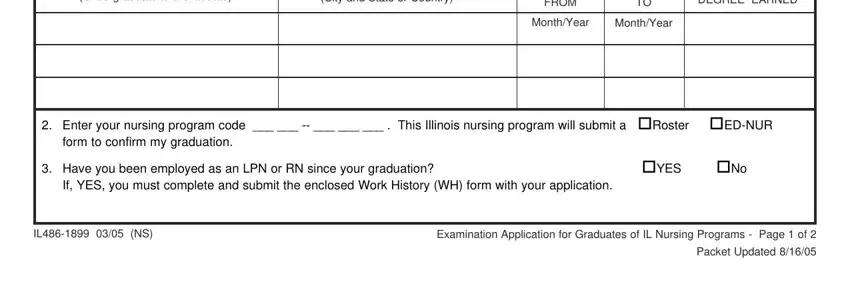
3. The following part will be focused on Undergraduate and Graduate, City and State or Country, FROM, DEGREE EARNED, MonthYear, MonthYear, Enter your nursing program code, form to confirm my graduation, Have you been employed as an LPN, YES No, If YES you must complete and, IL NS, Examination Application for, and Packet Updated - type in each of these blanks.
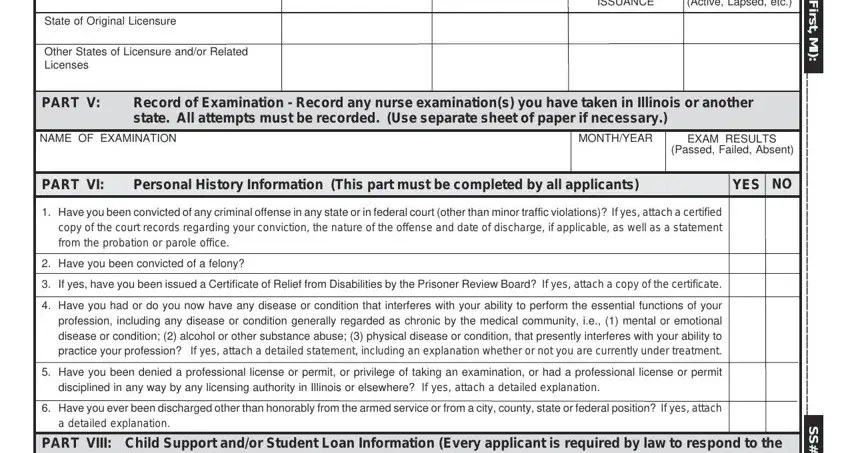
4. Completing DATE OF ISSUANCE, LICENSE STATUS Active Lapsed etc, State of Original Licensure, Other States of Licensure andor, PART V, Record of Examination Record any, NAME OF EXAMINATION, MONTHYEAR, EXAM RESULTS, Passed Failed Absent, PART VI, Personal History Information This, YES, Have you been convicted of any, and Have you been convicted of a is paramount in the next stage - ensure that you don't rush and be attentive with every single field!
5. And finally, this last subsection is what you have to complete before finalizing the form. The blank fields at this stage are the following: PART VIII Child Support andor, Child Support Information This, following questions, In accordance with Illinois, Are you more than days delinquent, Yes, In accordance with Illinois, Are you in default on an, Yes, PART VIII, Certifying Statement, Under penalties of perjury I, Signature of Applicant, Date, and I UNDERSTAND THAT FEES ARE NOT.
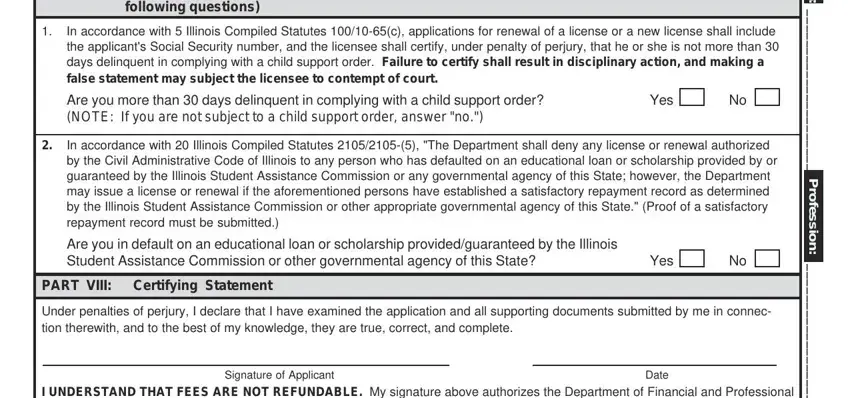
Be extremely attentive when completing In accordance with Illinois and Date, as this is the section in which many people make mistakes.
Step 3: Revise the information you have entered into the blank fields and then hit the "Done" button. Make a free trial option with us and obtain immediate access to licensee - which you may then make use of as you want inside your personal cabinet. FormsPal offers secure form editing with no personal data recording or any sort of sharing. Rest assured that your data is safe with us!