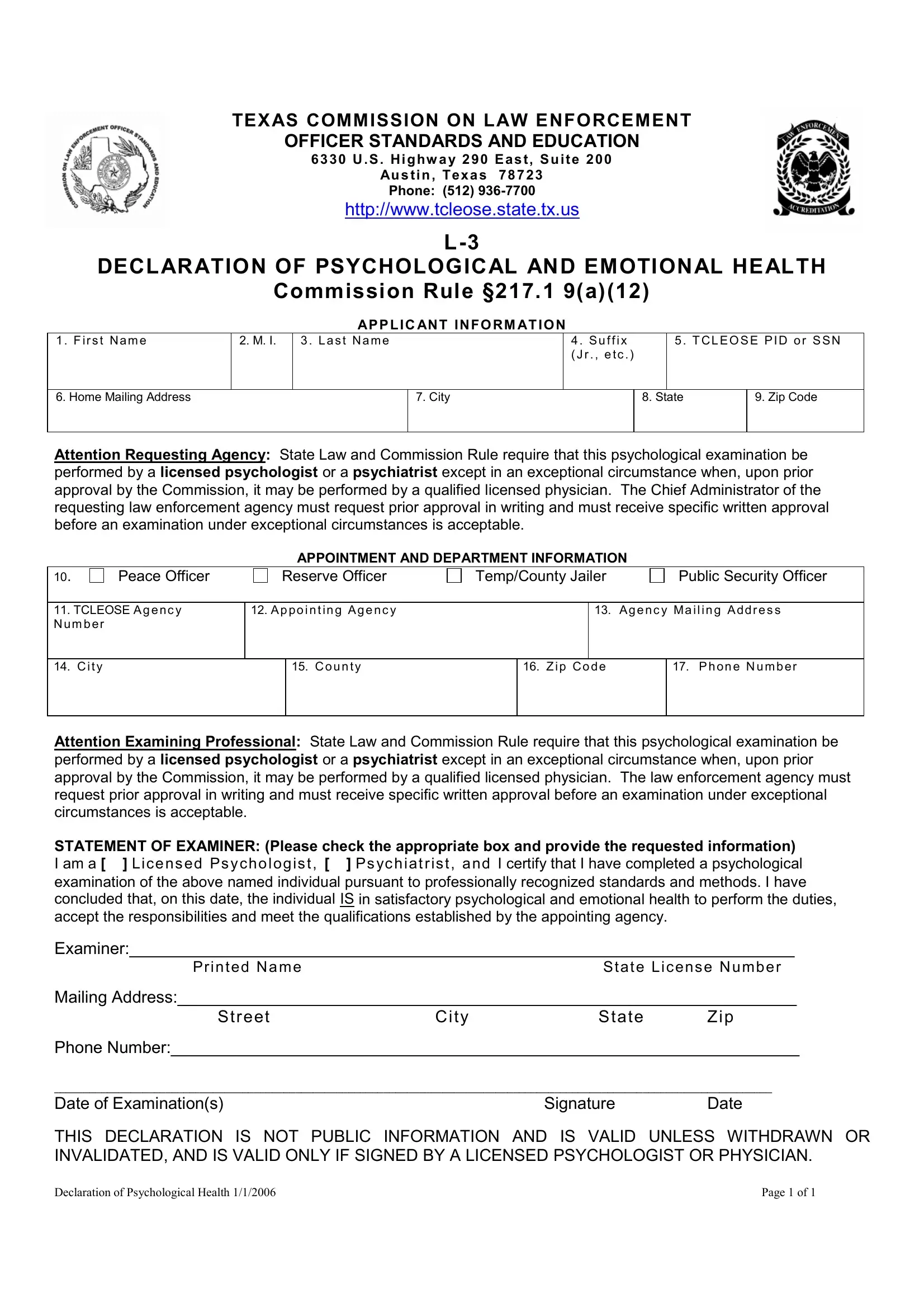
In the realm of law enforcement, the health and readiness of its officers not only impacts individual careers but also the broader community's safety and trust in its police force. The L-3 Declaration of Psychological and Emotional Health, mandated by the Texas Commission on Law Enforcement Officer Standards and Education, is a crucial document in this context. This form serves as a formal attestation to a prospective or current officer’s psychological and emotional fitness for duty. It outlines a process whereby psychological examinations are conducted by authorized professionals—specifically, licensed psychologists, psychiatrists, or, in rare instances with prior approval, qualified licensed physicians. The instructions detail the necessity for these evaluations to be conducted following professionally recognized standards, ensuring the individual's capability to undertake the responsibilities and duties assigned by their appointing agency. Importantly, this form is not public information, emphasizing the confidentiality associated with such sensitive assessments. Moreover, the validation of this document, contingent upon the signature of a licensed professional, underpins its importance in the law enforcement certification process, reflecting the commitment to maintaining a force capable of upholding the law effectively and empathetically.
| Question | Answer |
|---|---|
| Form Name | Form L 3 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | L 3 Form harris county l3 tests form |
TEXAS COMMISSION ON LAW ENFORCEMENT
OFFICER STANDARDS AND EDUCATION
6330 U.S. Highw ay 290 East, Suite 200
Austin, Texas 78723
Phone: (512)
http://www.tcleose.state.tx.us
DECLARATION OF PSYCHOLOGICAL AND EMOTIONAL HEALTH
Commission Rule §217.1 9(a)(12)
APPLIC ANT INFORM ATION
1. F irst Name
2. M. I.
3. Last Name
4. Suffix (Jr., etc.)
5. T CLEOSE PID or SSN
6. Home Mailing Address
7. City
8. State
9. Zip Code
Attention Requesting Agency: State Law and Commission Rule require that this psychological examination be performed by a licensed psychologist or a psychiatrist except in an exceptional circumstance when, upon prior approval by the Commission, it may be performed by a qualified licensed physician. The Chief Administrator of the requesting law enforcement agency must request prior approval in writing and must receive specific written approval before an examination under exceptional circumstances is acceptable.
APPOINTMENT AND DEPARTMENT INFORMATION
10. |
Peace Officer |
Reserve Officer |
Temp/County Jailer |
|
Public Security Officer |
|||
|
|
|
|
|
|
|
|
|
11. TCLEOSE Agenc y |
12. Appointing Agenc y |
|
|
13. |
Agenc y Mailing Addres s |
|||
Num ber |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
14. City |
|
|
15. County |
|
16. Zip Code |
|
17. Phone Number |
|
|
|
|
|
|
|
|
|
|
Attention Examining Professional: State Law and Commission Rule require that this psychological examination be performed by a licensed psychologist or a psychiatrist except in an exceptional circumstance when, upon prior approval by the Commission, it may be performed by a qualified licensed physician. The law enforcement agency must request prior approval in writing and must receive specific written approval before an examination under exceptional circumstances is acceptable.
STATEMENT OF EXAMINER: (Please check the appropriate box and provide the requested information) I am a [ ] Licensed Psychologist, [ ] Psychiatrist, and I certify that I have completed a psychological examination of the above named individual pursuant to professionally recognized standards and methods. I have concluded that, on this date, the individual IS in satisfactory psychological and emotional health to perform the duties, accept the responsibilities and meet the qualifications established by the appointing agency.
Examiner:________________________________________________________________________
Printed NameState License Number
Mailing Address:___________________________________________________________________
StreetCityState Zip
Phone Number:____________________________________________________________________
__________________________________________________________________________________________________________________________
Date of Examination(s) |
Signature |
Date |
THIS DECLARATION IS NOT PUBLIC INFORMATION AND IS VALID UNLESS WITHDRAWN OR INVALIDATED, AND IS VALID ONLY IF SIGNED BY A LICENSED PSYCHOLOGIST OR PHYSICIAN.
Declaration of Psychological Health 1/1/2006 |
Page 1 of 1 |