

It is possible to work with Form Lb 0973 without difficulty by using our PDFinity® online PDF tool. FormsPal team is committed to making sure you have the perfect experience with our tool by constantly presenting new features and improvements. Our editor is now a lot more helpful thanks to the most recent updates! Currently, filling out PDF documents is a lot easier and faster than ever before. To get started on your journey, consider these simple steps:
Step 1: Click on the "Get Form" button above on this webpage to open our PDF editor.
Step 2: After you access the editor, you will find the form ready to be completed. Apart from filling out various blanks, you might also do other things with the form, that is adding your own words, modifying the initial text, inserting graphics, affixing your signature to the PDF, and a lot more.
When it comes to blank fields of this specific document, here's what you should do:
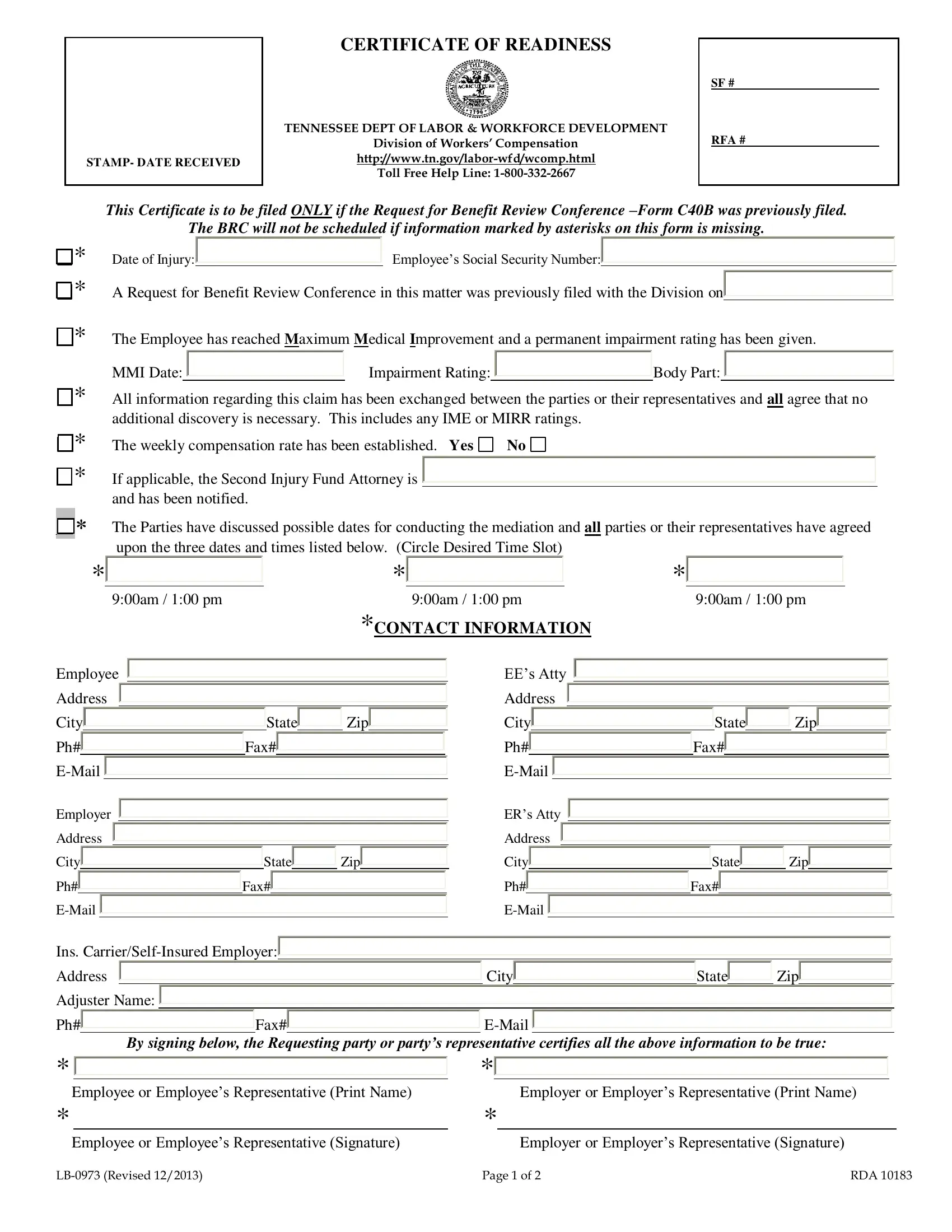
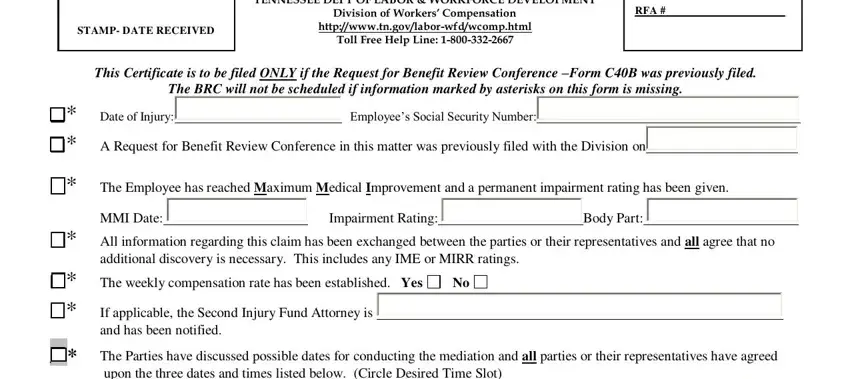
1. First of all, while completing the Form Lb 0973, beging with the form section containing following fields:
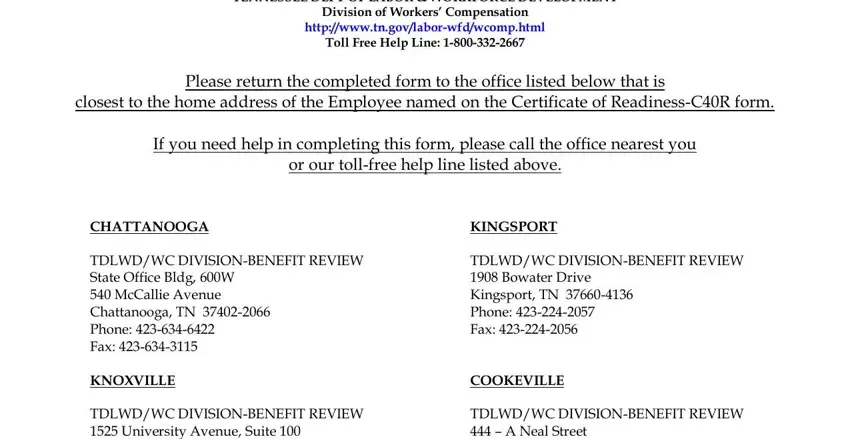
2. Once your current task is complete, take the next step – fill out all of these fields - TENNESSEE DEPT OF LABOR WORKFORCE, Division of Workers Compensation, httpwwwtngovlaborwfdwcomphtml, Toll Free Help Line, Please return the completed form, closest to the home address of the, If you need help in completing, or our tollfree help line listed, CHATTANOOGA TDLWDWC, KINGSPORT TDLWDWC DIVISIONBENEFIT, and COOKEVILLE TDLWDWC DIVISIONBENEFIT with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
People who work with this document often make mistakes while filling out KINGSPORT TDLWDWC DIVISIONBENEFIT in this section. Remember to revise everything you enter here.
Step 3: Right after you've looked over the details in the fields, just click "Done" to complete your form. Acquire the Form Lb 0973 after you join for a free trial. Easily gain access to the pdf form in your FormsPal account page, together with any edits and changes all synced! Whenever you work with FormsPal, it is simple to fill out documents without worrying about personal data leaks or data entries being shared. Our protected platform helps to ensure that your private information is kept safely.