
By using the online PDF editor by FormsPal, it is easy to complete or edit CLAIMANT right here. The editor is continually updated by our team, receiving powerful features and turning out to be greater. Should you be looking to start, this is what it's going to take:
Step 1: First of all, access the editor by clicking the "Get Form Button" above on this site.
Step 2: With the help of our online PDF editing tool, you're able to accomplish more than merely fill in blank fields. Express yourself and make your documents seem faultless with custom text added, or modify the file's original input to excellence - all accompanied by an ability to incorporate your own pictures and sign the PDF off.
It's straightforward to complete the form using this detailed guide! Here's what you have to do:
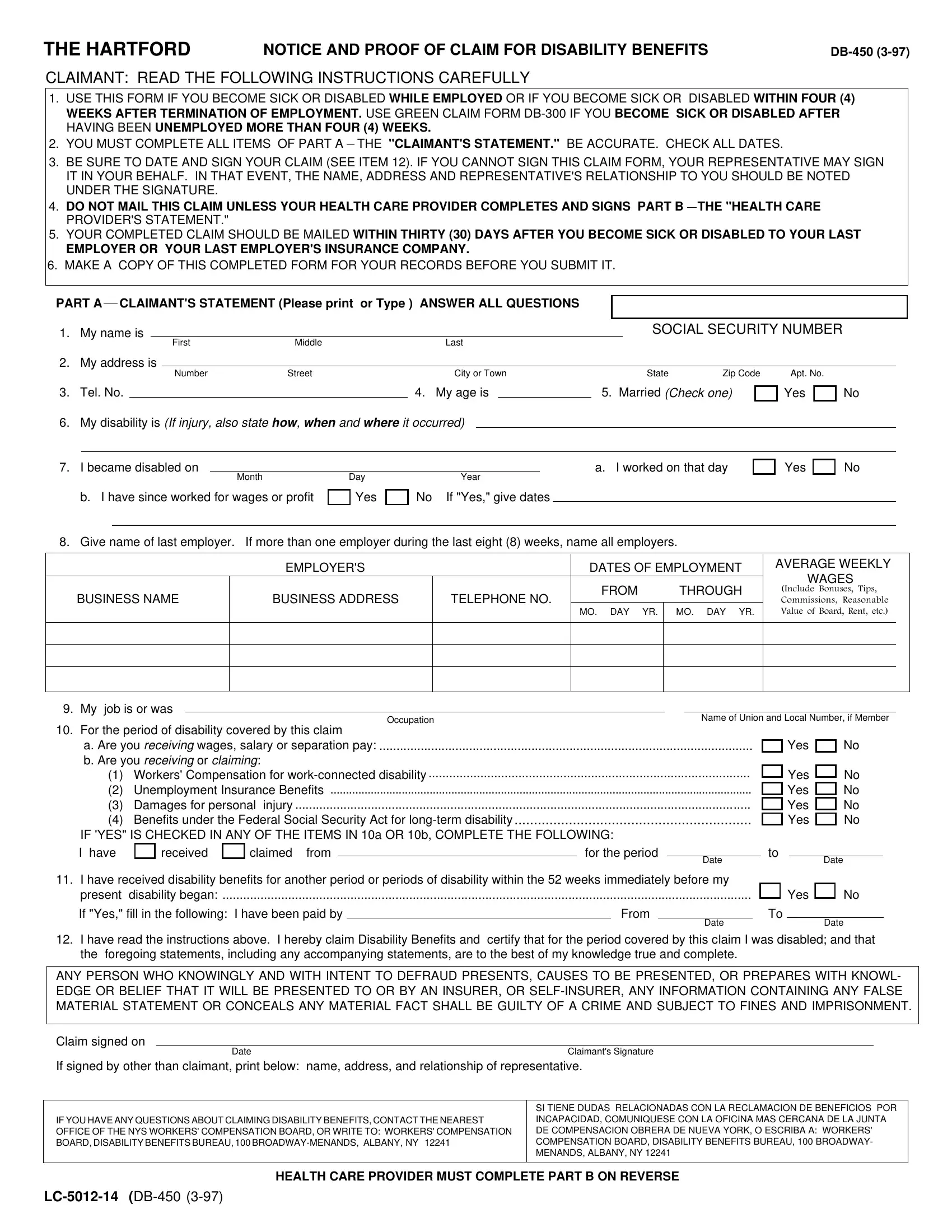
1. The CLAIMANT necessitates specific details to be typed in. Ensure that the next blank fields are finalized:
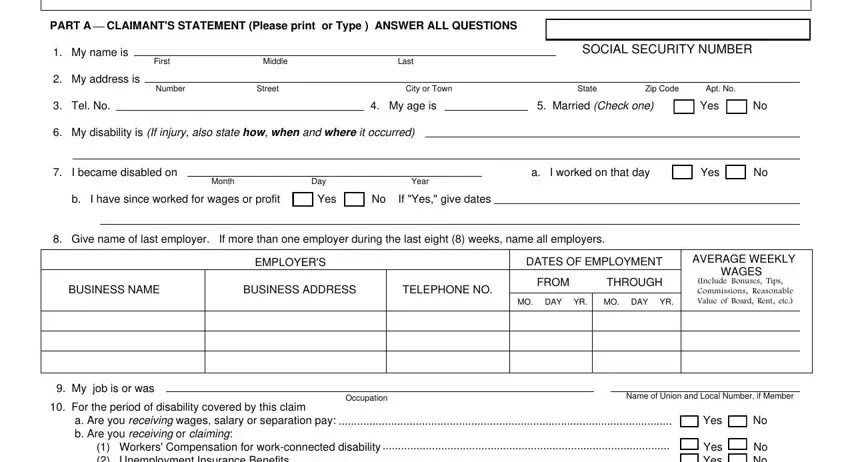
2. Once your current task is complete, take the next step – fill out all of these fields - For the period of disability, Yes Yes Yes Yes, No No No No, I have received claimed from, for the period, Date, Date, I have received disability, Yes, If Yes fill in the following I, From, Date, Date, I have read the instructions, and ANY PERSON WHO KNOWINGLY AND WITH with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
It's simple to make a mistake while completing the Yes, consequently make sure that you reread it before you decide to submit it.
3. Completing PART B HEALTH CARE PROVIDERS, Claimants Name, DiagnosisAnalysis a Claimants, b Objective Findings, Age, male, female, Diagnosis Code, Claimant hospitalized, Yes Operation indicated Yes, From, a Type, Enter dates for the following a, CPT Code, and Month is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
4. You're ready to fill out this next segment! Here you'll have all of these Health Care Providers Signature, Date, Tel No, Office Address, Number, Street, City or Town, State, Zip Code, Employers Statement, Employees Full Name as shown on, Policy Number SS Number, Employees Address Employees, Yes, and To To form blanks to fill out.
Step 3: Glance through what you've typed into the form fields and then click on the "Done" button. Go for a free trial option with us and gain immediate access to CLAIMANT - download, email, or edit from your FormsPal cabinet. We don't sell or share any information that you type in while dealing with documents at our website.