
Using PDF forms online is quite easy with this PDF tool. You can fill out the hartford form lc 7135 12 here painlessly. Our expert team is always endeavoring to improve the tool and insure that it is much easier for clients with its multiple functions. Enjoy an ever-evolving experience today! Here is what you'll want to do to get started:
Step 1: Click on the "Get Form" button above on this page to access our PDF editor.
Step 2: When you launch the file editor, you will see the form ready to be completed. Besides filling out various fields, you may also perform some other things with the Document, that is writing your own textual content, modifying the initial text, inserting illustrations or photos, putting your signature on the document, and more.
Pay attention while completing this form. Ensure each blank is completed accurately.
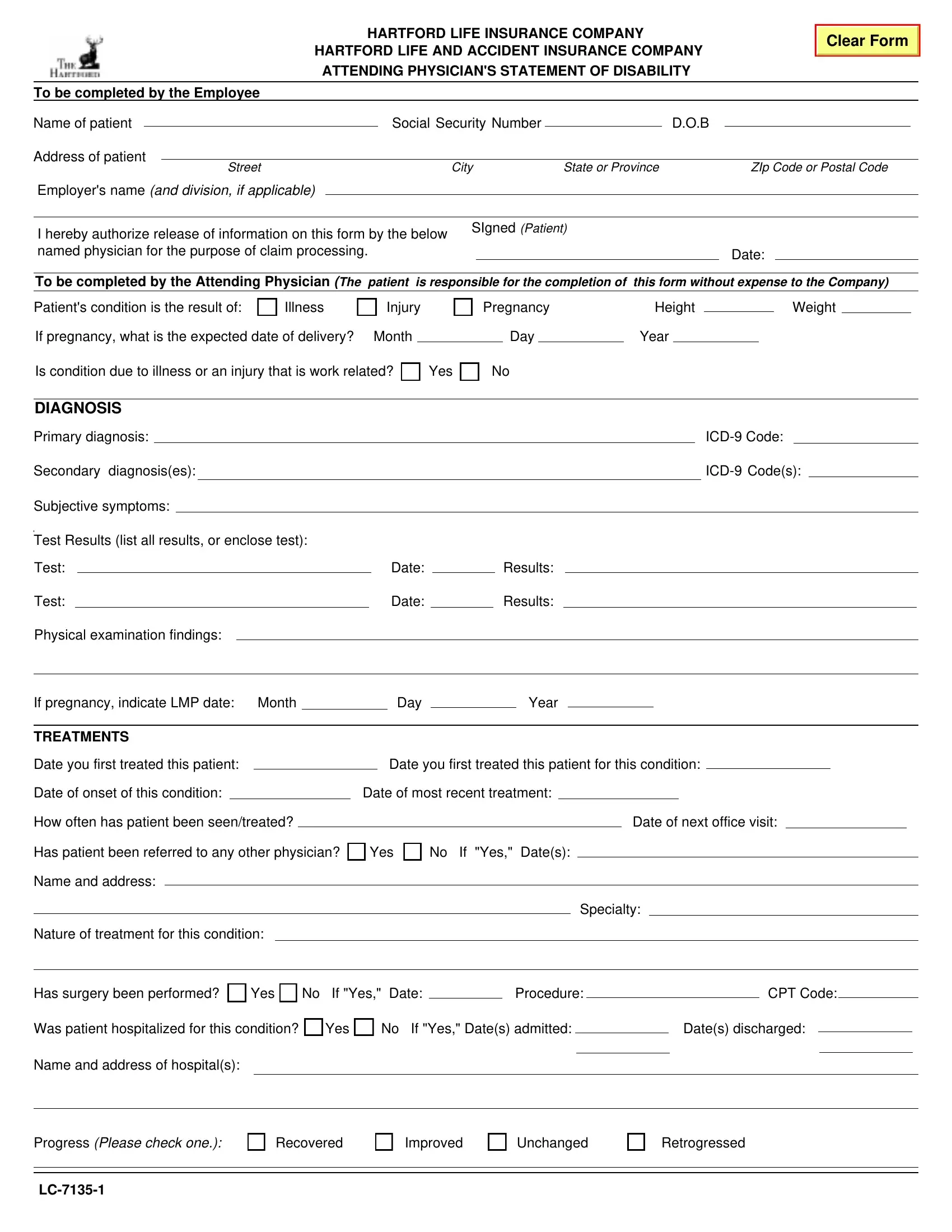
1. To start off, when completing the the hartford form lc 7135 12, start out with the part that has the subsequent fields:
2. Once the last section is completed, it is time to add the necessary particulars in Test, Test, Physical examination findings, Date, Date, Results, Results, If pregnancy indicate LMP date, Month, Day, Year, TREATMENTS, Date you first treated this patient, Date you first treated this, and Date of onset of this condition allowing you to go to the third step.
3. The following segment is rather simple, Has surgery been performed Yes No, CPT Code, Was patient hospitalized for this, No If Yes Dates admitted, Dates discharged, Name and address of hospitals, Progress Please check one Recovered, Improved, Unchanged, and Retrogressed - these blanks must be completed here.
Always be very attentive when filling in Improved and Retrogressed, because this is where a lot of people make errors.
4. The following subsection will require your involvement in the following areas: IMPAIRMENT If the patients ability, Standing, Walking, Sitting, Liftingcarrying, Reachingworking overhead, Pushing, Pulling, Driving, and Keyboard userepetitive hand motion. Make certain to fill in all requested information to move forward.
5. Lastly, the following last part is what you need to finish prior to finalizing the document. The blank fields here are the next: Keyboard userepetitive hand motion, If any other activities are, If the patients vision is impaired, Do you believe the patient is, What is the psychiatric impairment, Inadequate information to make, Essentially good functioning in, Slight difficulty in occupational, Moderate impairment in, Major impairment in several, Inability to function in almost, Date patient became unable to work, Day, Year, and If physical or psychiatric.
Step 3: Check the details you have typed into the blank fields and click on the "Done" button. Find your the hartford form lc 7135 12 the instant you register online for a free trial. Readily use the document within your FormsPal cabinet, with any modifications and adjustments all preserved! FormsPal offers secure document editing devoid of data recording or sharing. Rest assured that your details are in good hands here!