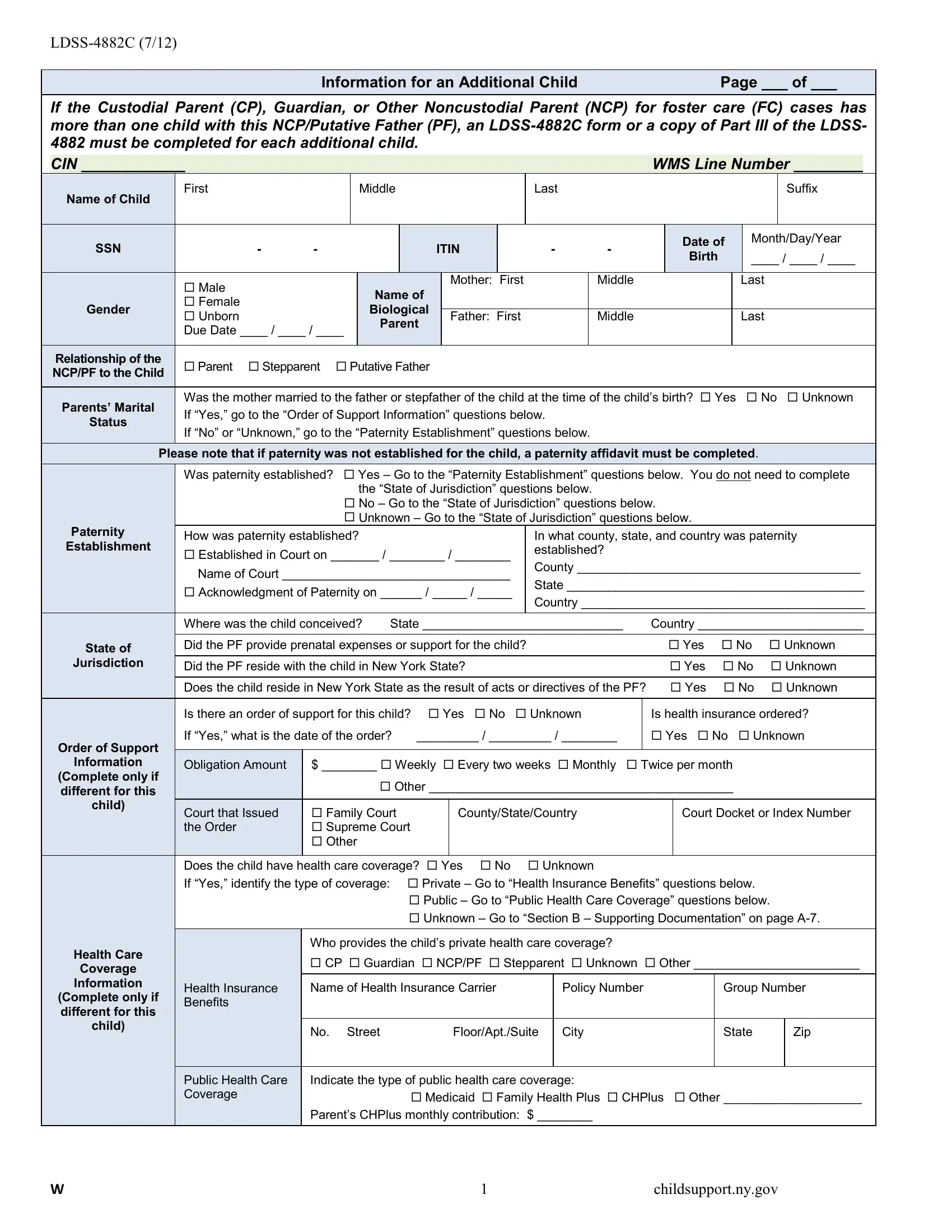
In today's complex family environments, effective management of child support and understanding the intricacies involved becomes imperative, especially when multiple children are concerned within the same case parameters. The LDSS-4882C form, a critical document released in July 2012, stands as an essential tool for custodial parents, guardians, and noncustodial parents in scenarios involving foster care. This form ensures that each child's unique needs and circumstances are thoroughly documented and considered in child support proceedings. It requires detailed information about additional children when a custodial parent (CP), guardian, or noncustodial parent (NCP) has more than one child with the same NCP or putative father (PF), demanding a separate completion for each child. The form encompasses a wide range of data, including but not limited to the child’s personal information, paternity establishment queries, state of jurisdiction considerations, order of support information, and specific sections on health care coverage. For foster care cases, there's an exclusive section that must be completed by the Commissioner or Designee, highlighting the form's versatility and the comprehensive nature of the data it seeks to collect to ensure the welfare of the child or children in question. Through the structured collection of this information, the form plays a pivotal role in facilitating the accurate assessment and enforcement of support obligations, thereby aiming to safeguard the best interests of each child involved.
| Question | Answer |
|---|---|
| Form Name | Form Ldss 4882C |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | nys form ldss 486t, ldss 4882c fillable form, ldss 486t, heap form ldss 3829 |
Information for an Additional ChildPage ___ of ___
If the Custodial Parent (CP), Guardian, or Other Noncustodial Parent (NCP) for foster care (FC) cases has more than one child with this NCP/Putative Father (PF), an
|
CIN ____________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
WMS Line Number ________ |
|
||||||||||||
|
|
|
|
First |
|
|
|
|
Middle |
|
|
|
|
|
|
|
Last |
|
|
|
|
|
|
|
|
|
|
|
|
Suffix |
|||
|
Name of Child |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date of |
Month/Day/Year |
|||||||
|
SSN |
- |
- |
|
|
|
|
|
|
ITIN |
|
|
- |
- |
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
Birth |
|
|
____ / ____ / ____ |
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Male |
|
|
|
|
|
Name of |
|
|
Mother: First |
|
|
|
Middle |
|
|
|
|
|
|
Last |
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
Female |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Gender |
|
|
|
|
|
|
Biological |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
Unborn |
|
|
|
|
|
|
|
Father: First |
|
|
|
Middle |
|
|
|
|
|
|
Last |
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
Parent |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
Due Date ____ / ____ / ____ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Relationship of the |
|
Parent Stepparent |
Putative Father |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
NCP/PF to the Child |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
Parents’ Marital |
|
Was the mother married to the father or stepfather of the child at the time of the child’s birth? Yes |
No Unknown |
|||||||||||||||||||||||||||||
|
|
If “Yes,” go to the “Order of Support Information” questions below. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
Status |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
If “No” or “Unknown,” go to the “Paternity Establishment” questions below. |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
Please note that if paternity was not established for the child, a paternity affidavit must be completed. |
|
|
|
|
||||||||||||||||||||||||||||
|
|
|
|
Was paternity established? Yes – Go to the “Paternity Establishment” questions below. You do not need to complete |
|||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
the “State of Jurisdiction” questions below. |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
No – Go to the “State of Jurisdiction” questions below. |
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
Unknown – Go to the “State of Jurisdiction” questions below. |
|
|
|
|
|
|
|
|||||||||||||||||||
|
Paternity |
|
How was paternity established? |
|
|
|
|
|
|
|
|
In what county, state, and country was paternity |
|||||||||||||||||||||
|
Establishment |
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
Established in Court on _______ / ________ / ________ |
established? |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
Name of Court _________________________________ |
County _________________________________________ |
||||||||||||||||||||||||||||
|
|
|
|
State ___________________________________________ |
|||||||||||||||||||||||||||||
|
|
|
|
Acknowledgment of Paternity on ______ / _____ / _____ |
|||||||||||||||||||||||||||||
|
|
|
|
Country _________________________________________ |
|||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
Where was the child conceived? |
State _____________________________ |
Country ________________________ |
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
State of |
|
|
Did the PF provide prenatal expenses or support for the child? |
|
|
|
|
|
|
Yes |
No |
Unknown |
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Jurisdiction |
|
|
Did the PF reside with the child in New York State? |
|
|
|
|
|
|
|
|
Yes |
No |
Unknown |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
Does the child reside in New York State as the result of acts or directives of the PF? |
|
Yes |
No |
Unknown |
|||||||||||||||||||||||||
|
|
|
|
Is there an order of support for this child? Yes |
No Unknown |
|
Is health insurance ordered? |
||||||||||||||||||||||||||
|
|
|
|
If “Yes,” what is the date of the order? |
_________ / _________ / ________ |
|
Yes No |
Unknown |
|||||||||||||||||||||||||
|
Order of Support |
|
|||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Information |
|
|
Obligation Amount |
|
$ ________ Weekly Every two weeks Monthly Twice per month |
|
|
|
|
|
||||||||||||||||||||||
|
(Complete only if |
|
|
|
|
|
|
|
|
Other ____________________________________________ |
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
different for this |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
child) |
|
|
Court that Issued |
|
Family Court |
|
|
|
|
County/State/Country |
|
|
Court Docket or Index Number |
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
|
|
the Order |
|
Supreme Court |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
Does the child have health care coverage? Yes |
No |
Unknown |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
If “Yes,” identify the type of coverage: |
Private – Go to “Health Insurance Benefits” questions below. |
|
|
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
Public – Go to “Public Health Care Coverage” questions below. |
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
Unknown – Go to “Section B – Supporting Documentation” on page |
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
Health Care |
|
|
|
|
Who provides the child’s private health care coverage? |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
CP Guardian NCP/PF Stepparent Unknown Other ________________________ |
||||||||||||||||||||||||||||
|
Coverage |
|
|
|
|
||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Information |
|
|
Health Insurance |
|
Name of Health Insurance Carrier |
|
|
Policy Number |
|
|
|
|
Group Number |
|||||||||||||||||||
|
(Complete only if |
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
|
Benefits |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
different for this |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
child) |
|
|
|
|
No. |
Street |
|
|
|
|
Floor/Apt./Suite |
|
City |
|
|
|
|
State |
|
|
Zip |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
Public Health Care |
|
Indicate the type of public health care coverage: |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
Coverage |
|
|
|
|
|
|
|
Medicaid Family Health Plus CHPlus Other ____________________ |
|||||||||||||||||||||
|
|
|
|
|
|
Parent’s CHPlus monthly contribution: $ ________ |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
W |
1 |
childsupport.ny.gov |
Part IV – Foster Care Information (Agency Use Only)
|
|
|
|
The Commissioner or Designee must complete this section on behalf of the social services |
|
||||||||||||||||
|
Foster Care |
|
|
||||||||||||||||||
|
|
|
district (SSD) or the Office of Children and Family Services (OCFS) Commissioner for a |
|
|||||||||||||||||
|
Referral |
|
|
|
|||||||||||||||||
|
|
|
child in Foster Care placement. |
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name of Child |
|
First |
|
|
Middle |
|
|
|
|
Last |
|
|
|
Suffix |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
Case Number |
|
Case Status |
|
|
|
|
|
|
Date of Referral |
|
|||||||
|
Case Information |
|
|
|
|
Opening |
|
Reopening |
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
Changes or Updates |
|
|
|
|
|
_______ / _______ / ________ |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Category |
|
What is the claiming category? |
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
Voluntary |
Placement Date |
|
|
|
|
Cost of Care |
|
|
|
|
|
|
|||||
|
Type of Placement |
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
Court Ordered |
_________ / _________ / _________ |
|
$ ___________ Per: Day Week Month Year |
|
|||||||||||||||
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Name of Agency, |
|
|
County |
|
|
Agency Name |
|
|
|
|
|
Type of Facility |
|
|
|
|
||||
|
Facility, Foster |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Boarding Home |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Placement Address |
|
No. |
Street |
Floor/Apt./Suite |
City |
|
|
|
|
|
|
|
State |
|
|
Zip |
|
|||
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
Is an adoption subsidy received on behalf of the child? |
Does the subsidy include Medicaid? |
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
||||||||||||||
|
Subsidy |
|
|
Yes |
No |
|
|
|
|
Yes |
No |
|
|
|
|
|
|
||||
|
Information |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Subsidy Amount and When It Is Paid |
$ ________________ Per: |
|
Week |
Month |
Year |
|
||||||||||||
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
Name |
|
|
|
|
|
|
Phone Number |
|
|
|
|
|
|
||||
|
Case Manager |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
( |
|
) |
|
|
Ext. |
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
I am applying for Child Support Services as the Commissioner or Designee and this is a |
|
||||||||||||||||
|
Application for |
|
|
Foster Care referral. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Child Support |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Services |
|
|
Signature of Commissioner/Designee ________________________________________________ |
|
||||||||||||||||
|
|
|
|
Date ____________________________________________________________________________________________ |
|
||||||||||||||||
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
W |
2 |
childsupport.ny.gov |