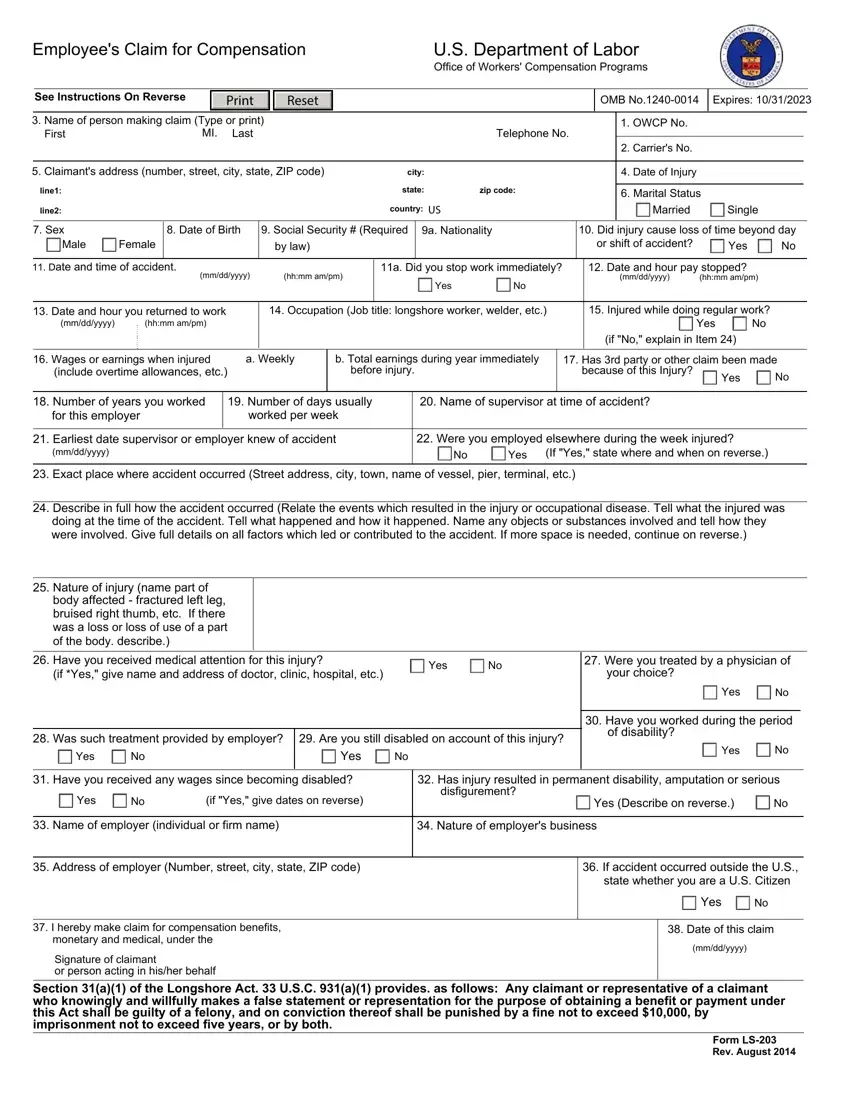
Employee's Claim for Compensation |
|
|
|
|
U.S. Department of Labor |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Office of Workers' Compensation Programs |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
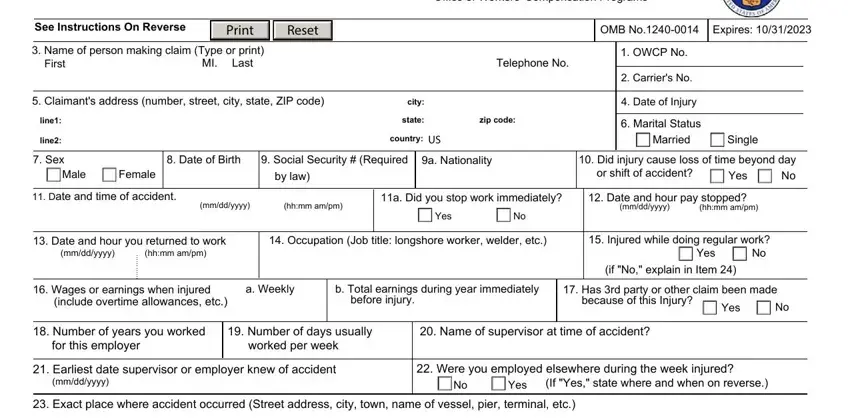
See Instructions On Reverse |
|
|
Print |
|
|
Reset |
|
|
|
|
|
|
|
|
|
|
OMB No.1240-0014 |
|
Expires: 10/31/2023 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3. Name of person making claim (Type or print) |
|
|
|
|
|
|
|
|
|
|
|
1. OWCP No. |
|
|
|
|
|
|
|
First |
|
MI. |
Last |
|
|
|
|
|
|
|
|
Telephone No. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. Carrier's No. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5. Claimant's address (number, street, city, state, ZIP code) |
|
|
city: |
|
|
|
|
|
|
4. Date of Injury |
|
|
|
|
|
|
|
line1: |
|
|
|
|
|
|
|
|
|
|
state: |
zip code: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6. Marital Status |
|
|
|
|
|
line2: |
|
|
|
|
|
|
|
|
|
|
country: US |
|
|
|
|
|
|
Married |
|
Single |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7. Sex |
|
8. Date of Birth |
9. Social Security # (Required |
9a. Nationality |
|
10. Did injury cause loss of time beyond day |
|
Male |
Female |
|
|
|
|
|
|
by law) |
|
|
|
|
|
|
|
|
|
|
or shift of accident? |
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
11. Date and time of accident. |
|
|
|
(hh:mm am/pm) |
|
11a. Did you stop work immediately? |
|
|
12. Date and hour pay stopped? |
|
|
|
|
|
|
|
(mm/dd/yyyy) |
|
|
|
|
|
Yes |
No |
|
|
|
|
(mm/dd/yyyy) |
(hh:mm am/pm) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
13. Date and hour you returned to work |
|
14. Occupation (Job title: longshore worker, welder, etc.) |
|
|
15. Injured while doing regular work? |
|
(mm/dd/yyyy) |
(hh:mm am/pm) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(if "No," explain in Item 24) |
|
|
|
|
16. Wages or earnings when injured |
a. Weekly |
b. Total earnings during year immediately |
|
17. Has 3rd party or other claim been made |
|
(include overtime allowances, etc.) |
|
|
|
|
before injury. |
|
|
|
|
because of this Injury? |
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
18. Number of years you worked |
|
19. Number of days usually |
|
20. Name of supervisor at time of accident? |
|
|
|
|
|
|
|
for this employer |
|
worked per week |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
21. Earliest date supervisor or employer knew of accident |
|
|
|
22. Were you employed elsewhere during the week injured? |
|
|
|
|
|
(mm/dd/yyyy) |
|
|
|
|
|
|
|
|
|
|
|
|
No |
Yes (If "Yes," state where and when on reverse.) |
|
23.Exact place where accident occurred (Street address, city, town, name of vessel, pier, terminal, etc.)
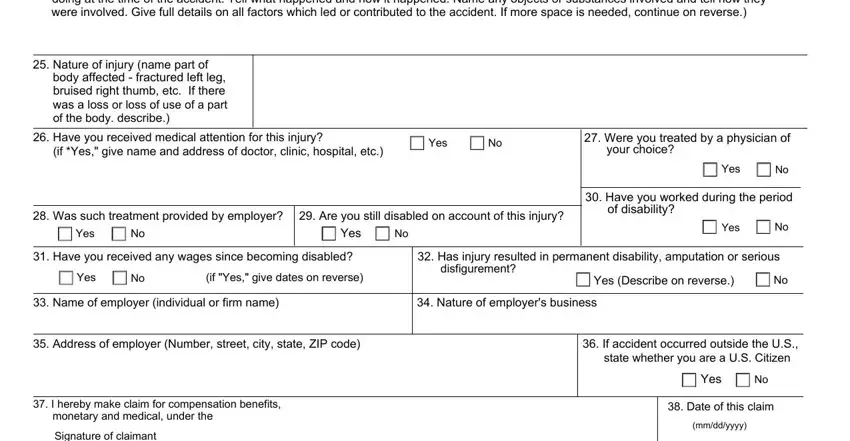
24.Describe in full how the accident occurred (Relate the events which resulted in the injury or occupational disease. Tell what the injured was doing at the time of the accident. Tell what happened and how it happened. Name any objects or substances involved and tell how they were involved. Give full details on all factors which led or contributed to the accident. If more space is needed, continue on reverse.)
25.Nature of injury (name part of body affected - fractured left leg, bruised right thumb, etc. If there was a loss or loss of use of a part of the body. describe.)
26. |
Have you received medical attention for this injury? |
|
Yes |
No |
|
27. Were you treated by a physician of |
|
|
|
(if *Yes," give name and address of doctor, clinic, hospital, etc.) |
|
|
your choice? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
30. Have you worked during the period |
|
|
|
|
|
|
|
|
|
|
|
of disability? |
|
|
|
28. |
Was such treatment provided by employer? |
29. Are you still disabled on account of this injury? |
|
No |
|
|
|
Yes |
|
|
|
Yes |
No |
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
31. |
Have you received any wages since becoming disabled? |
|
32. Has injury resulted in permanent disability, amputation or serious |
|
|
|
Yes |
No |
(if "Yes," give dates on reverse) |
|
disfigurement? |
Yes (Describe on reverse.) |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
33. Name of employer (individual or firm name) |
|
|
34. Nature of employer's business |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
35. Address of employer (Number, street, city, state, ZIP code)
36.If accident occurred outside the U.S., state whether you are a U.S. Citizen
 Yes
Yes  No
No
37.I hereby make claim for compensation benefits, monetary and medical, under the
Signature of claimant
or person acting in his/her behalf
38. Date of this claim
(mm/dd/yyyy)
Section 31(a)(1) of the Longshore Act. 33 U.S.C. 931(a)(1) provides. as follows: Any claimant or representative of a claimant who knowingly and willfully makes a false statement or representation for the purpose of obtaining a benefit or payment under this Act shall be guilty of a felony, and on conviction thereof shall be punished by a fine not to exceed $10,000, by imprisonment not to exceed five years, or by both.
Form LS-203
Rev. August 2014
Instructions
• Use this form to file a claim under any one of the following laws:
Longshore and Harbor Workers' Compensation Act
Defense Base Act
Outer Continental Shelf Lands Act
Nonappropriated Fund Instrumentalities Act
- Applicant may leave items 1. and 2. blank.
Except as noted below, a claim may be filed within one year after the injury or death (33 U.S.C. 913(a)). If compensation has been paid without an
award, a claim may be filed within one year after the last payment. The time for filing a claim does not begin to run until the employee or beneficiary
knows, or should have known by the exercise of reasonable diligence, of the relationship between the employment and the injury. Persons are not
required to respond to this collection of information unless it displays a currently valid OMB control number. The information will be used to determine
an injured worker's entitlement to compensation and medical benefits.
In case of hearing loss, a claim may be filed within one year after receipt by an employee of an audiogram, with the accompanying report thereon, indicating that the employee has suffered a loss of hearing.
In cases involving occupational disease which does not immediately result in death or disability, a claim may be filed within two years after the
employee or claimant becomes aware, or in the exercise of reasonable diligence or by reason of medical advice should have been aware, of the relationship between the employment, the disease, and the death or disability.
To file a claim for compensation benefits, complete and sign this form.
If you have already been assigned an OWCP Case Number, please include your OWCP case number and submit electronically to the file through the DLHWC’s Secure Electronic Access Portal (SEAPortal) https://seaportal.dol.gov/portal/?program_name=LS. Alternatively, to submit the claim by mail, please be sure to include your case number and mail to the Central Mail Receipt site at the address shown below.
If this is a new claim, and you do not have an OWCP Case Number, please submit the form through the Case Create Fax Number (202) 513-6814. Alternatively, to submit the "case create" form by mail, please send it to the address below:
U.S. Department of Labor
Office of Workers’ Compensation Programs
Division of Federal Employees’, Longshore and Harbor Workers' Compensation
400 West Bay Street, Suite 63A, Box 28
Jacksonville, FL 32202
Use the space below to continue answers. Please number each answer to correspond to the number of the item being continued.
Privacy Act Notice
In accordance with the Privacy Act of 1974, as amended (5 U.S.C. 552a) you are hereby notified that (1) the Longshore and Harbor Workers' Compensation Act, as amended and extended (33 U.S.C. 901 et seq.) (LHWCA) is administered by the Office of Workers' Compensation Programs of the U.S. Department of Labor, which receives and maintains personal information on claimants and their immediate families. (2) Information which the Office has will be used to determine eligibility for and the amount of benefits payable under the LHWCA. (3) Information may be given to the employer which employed the claimant at the time of injury, or to the insurance carrier or other entity which secured the employer's compensation liability. (4) Information may be given to physicians and other medical service providers for use in providing treatment or medical/vocational rehabilitation, making evaluations and for other purposes relating to the medical management of the claim. (5) Information may be given to the Department of Labor's Office of Administrative Law Judges (OALJ), or other person, board or organization, which is authorized or required to render decisions with respect to the claim or other matter arising in connection with the claim.
(6)Information may be given to the Federal, state and local agencies for law enforcement purposes, to obtain information relevant to a decision under the LHWCA, to determine whether benefits are being or have been paid properly, and where appropriate, to pursue salary/administrative offset and debt collection actions required or permitted by law. (7) Disclosure of the claimant's Social Security Number (SSN) or tax identifying number (TIN) on this form is mandatory. The SSN and/or TIN and other information maintained by the Office may be used for identification, and for other purposes authorized by law. (8) Failure to disclose all requested information may delay the processing of the claim, the payment of benefits, or may result in an unfavorable decision or reduced level of benefits.
Note: The notice applies to all forms requesting information that you might receive from the Office in connection with the processing and/or adjudication of the claim you filed under the LHWCA and related statutes.
Public Burden Statement
According to the Paperwork Reduction Act of 1995, no persons are required to respond to a collection of information unless such collection displays a valid OMB control number. Public reporting burden for this collection of information is estimated to average 15 minutes per response, including time for reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information. Use of this form is optional, however furnishing the information is required in order to obtain and/or retain benefits. ( 33 U.S.C.913(a) ). Send comments regarding the burden estimate or any other aspect of this collection of information, including suggestions for reducing this burden, to the U.S. Department of Labor, 200 Constitution Avenue, NW, Room S-3229, Washington, D.C. 20210, and reference the OMB Control Number.
DO NOT SEND THE COMPLETED FORM TO THIS OFFICE