Creating the form 203 file is a breeze with this PDF editor. Follow the following steps to obtain the document instantly.
Step 1: First, hit the orange button "Get Form Now".
Step 2: At the moment you are on the file editing page. You may change and add text to the file, highlight words and phrases, cross or check specific words, insert images, put a signature on it, erase needless fields, or eliminate them entirely.
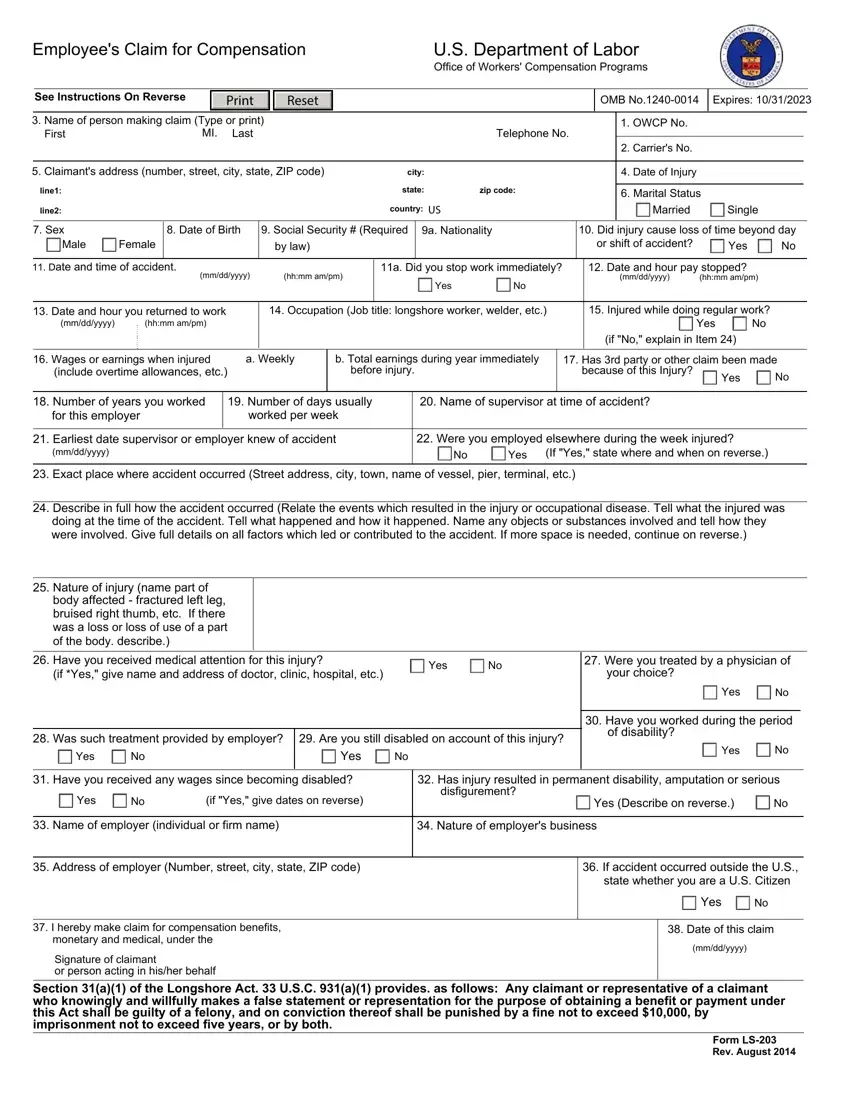
Fill out the form 203 PDF by typing in the details necessary for each individual section.
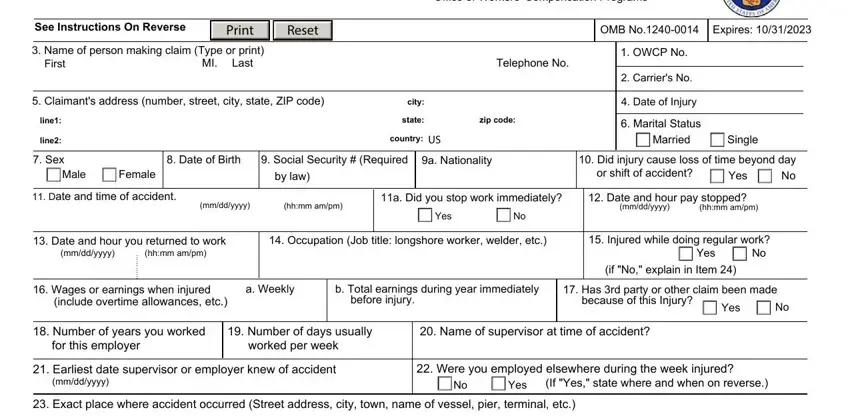
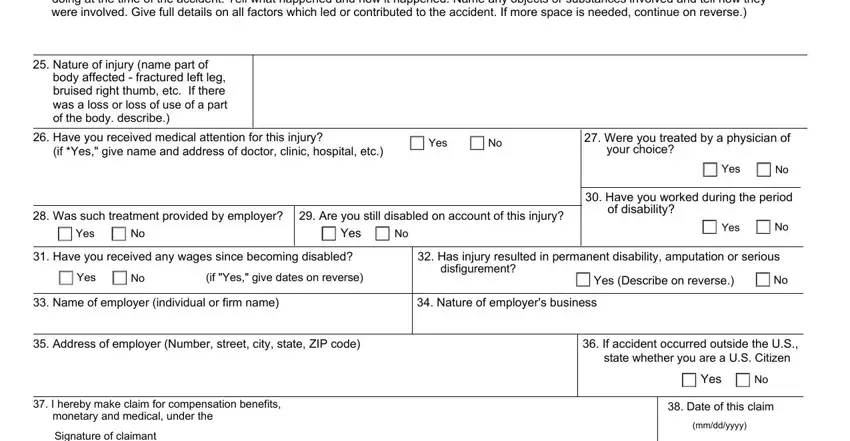
Fill out the Describe in full how the accident, Nature of injury name part of, body affected fractured left leg, Have you received medical, if Yes give name and address of, Yes, Were you treated by a physician of, your choice, Was such treatment provided by, Are you still disabled on account, Yes, Yes, Yes, Have you worked during the period, and of disability fields with any information that can be requested by the application.
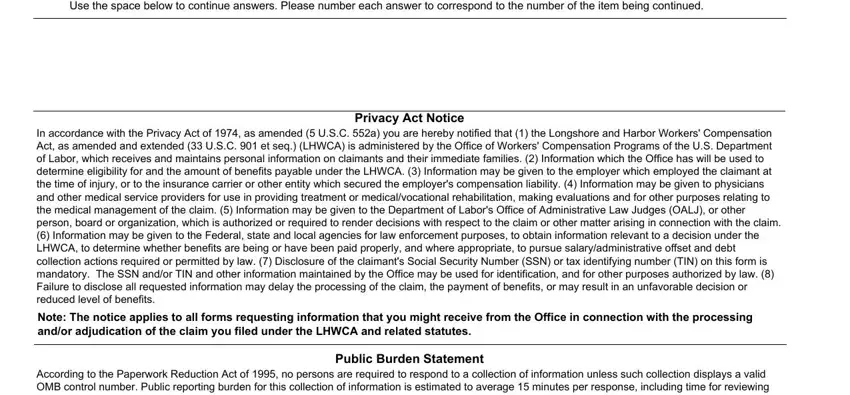
You'll have to note specific details in the section Use the space below to continue, Privacy Act Notice In accordance, Note The notice applies to all, According to the Paperwork, and Public Burden Statement.
Step 3: Press the button "Done". Your PDF file can be exported. It's possible to download it to your laptop or email it.
Step 4: In order to prevent any sort of troubles down the road, you will need to generate around a couple of copies of the document.
