
With the online PDF editor by FormsPal, you may complete or change form 1008 right here. Our professional team is constantly working to develop the editor and ensure it is even faster for people with its extensive functions. Capitalize on present-day revolutionary possibilities, and find a trove of new experiences! It just takes a few simple steps:
Step 1: Access the form in our editor by pressing the "Get Form Button" at the top of this webpage.
Step 2: This editor will let you change your PDF document in a range of ways. Improve it by adding any text, correct what's already in the PDF, and put in a signature - all when you need it!
It is actually easy to fill out the document with this detailed tutorial! Here's what you have to do:
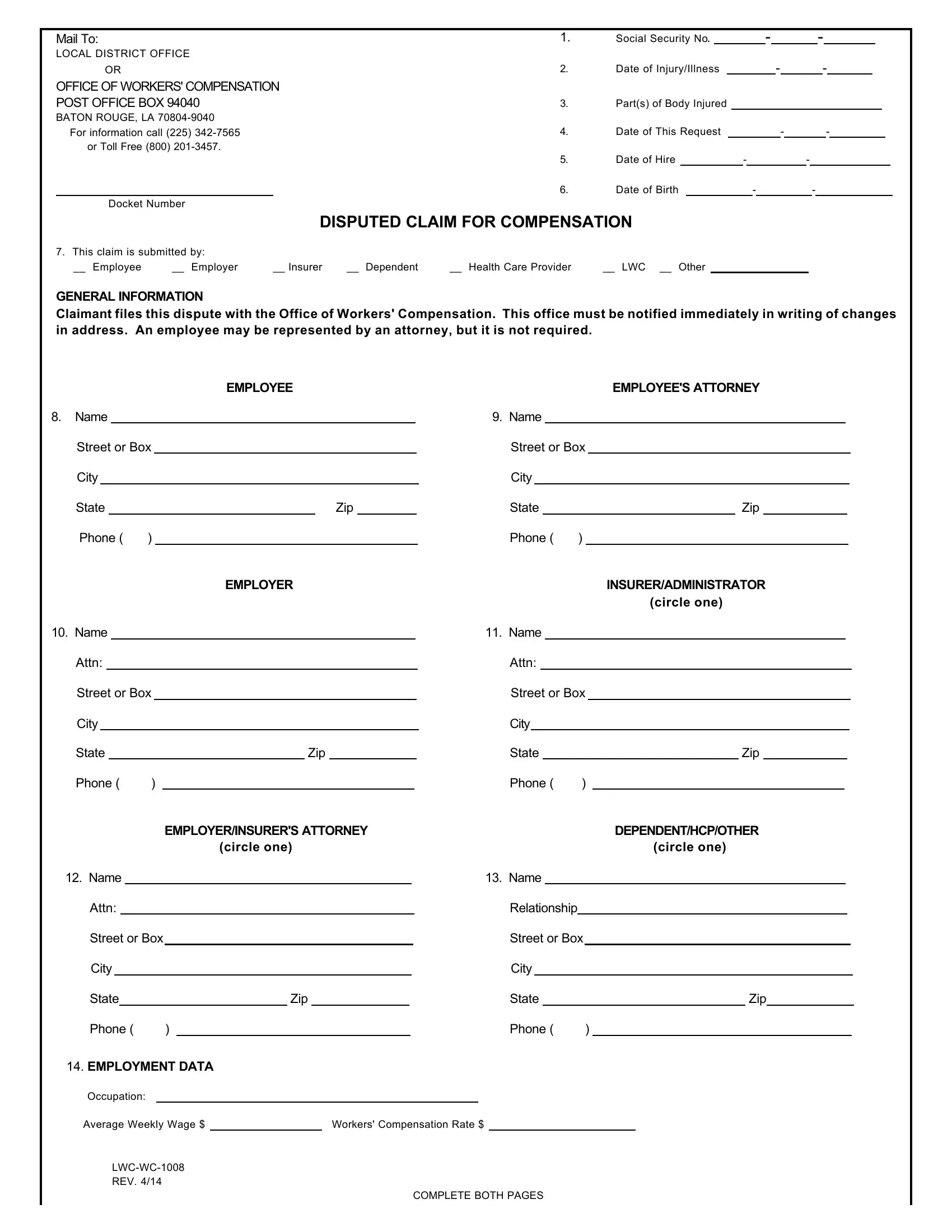
1. You need to fill out the form 1008 properly, therefore be mindful when filling in the sections that contain these blank fields:
2. Right after completing the last part, head on to the subsequent stage and fill out all required details in all these blank fields - Street or Box, Street or Box, City, City, State Zip, State Zip, Phone, Phone, EMPLOYER, INSURERADMINISTRATOR, circle one, Name, Name, Attn, and Attn.
3. This 3rd step is considered fairly straightforward, Name, Name, Attn, Relationship, Street or Box, Street or Box, City, City, State Zip, State Zip, Phone, Phone, EMPLOYMENT DATA, Occupation, and Average Weekly Wage Workers - these blanks will need to be filled in here.
People often make mistakes while filling out Name in this part. Be sure you read twice everything you type in here.
4. The following section will require your involvement in the subsequent places: A ACCIDENT DATA, Date time and place of accident, Parish of Residence at time of, Accident reported on to whose, Describe the accident and injury, List the names addresses telephone, B MEDICAL DATA, and State the names addresses and. Be sure to provide all required information to go forward.
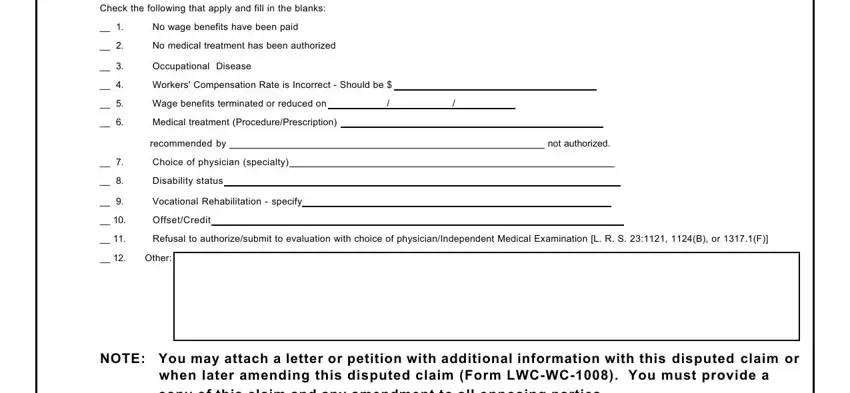
5. The last point to finalize this PDF form is essential. Make sure that you fill in the mandatory form fields, which includes Check the following that apply and, No wage benefits have been paid, No medical treatment has been, Occupational Disease, Workers Compensation Rate is, Wage benefits terminated or, Medical treatment, recommended by not authorized, Choice of physician specialty, Disability status, Vocational Rehabilitation specify, OffsetCredit, Refusal to authorizesubmit to, Other, and NOTE You may attach a letter or, before finalizing. Failing to accomplish that can give you a flawed and probably unacceptable form!
Step 3: After you've reread the details entered, simply click "Done" to finalize your form. Make a free trial subscription with us and get direct access to form 1008 - readily available inside your FormsPal account. FormsPal guarantees your information confidentiality via a secure system that never saves or distributes any kind of private information used in the PDF. Feel safe knowing your documents are kept protected whenever you use our services!