
Using PDF forms online is actually very simple using our PDF tool. You can fill out Los here effortlessly. Our team is ceaselessly endeavoring to develop the tool and help it become much better for clients with its extensive functions. Enjoy an ever-improving experience today! It just takes a couple of simple steps:
Step 1: Firstly, access the pdf editor by pressing the "Get Form Button" above on this site.
Step 2: The tool offers the ability to modify almost all PDF files in many different ways. Modify it by adding your own text, correct what is already in the file, and add a signature - all within a few mouse clicks!
With regards to the fields of this precise form, here's what you should know:
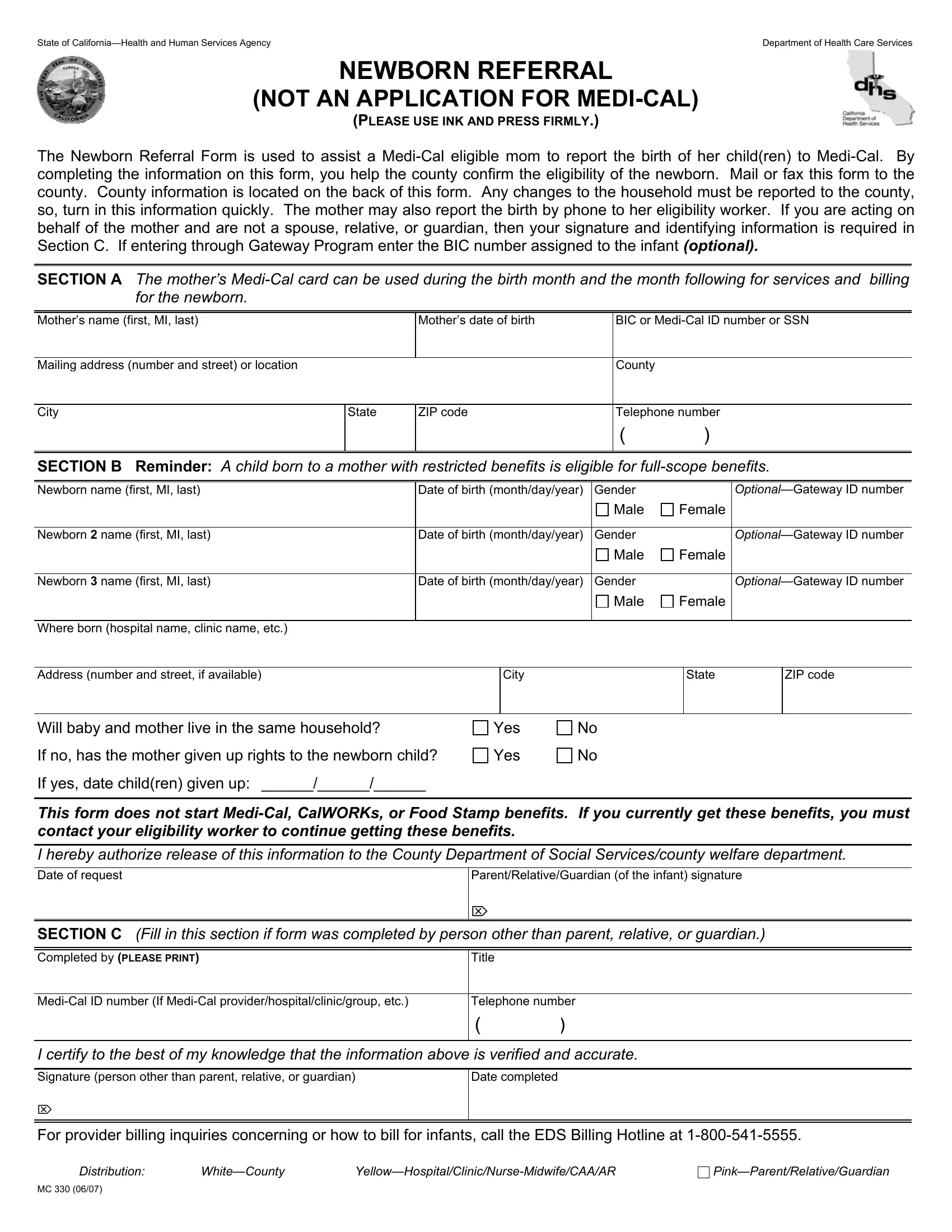
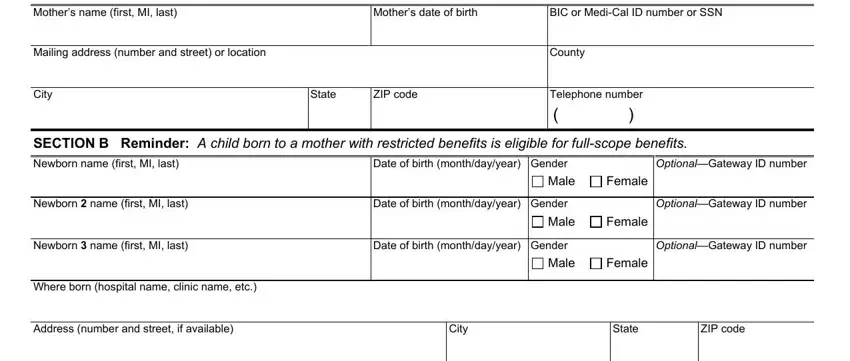
1. Begin filling out your Los with a selection of necessary blanks. Collect all the required information and make certain there's nothing missed!
2. The next stage is usually to submit all of the following blanks: Will baby and mother live in the, If no has the mother given up, If yes date children given up, Yes, Yes, This form does not start MediCal, I hereby authorize release of this, ParentRelativeGuardian of the, SECTION C Fill in this section if, Completed by PLEASE PRINT, Title, MediCal ID number If MediCal, Telephone number, I certify to the best of my, and Signature person other than parent.
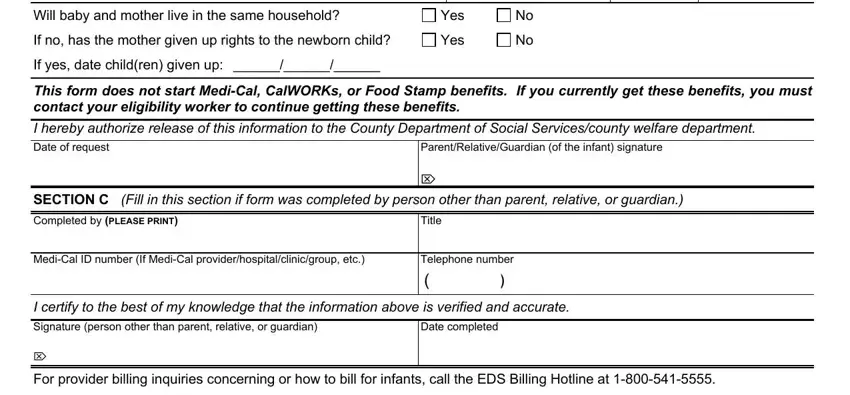
As to SECTION C Fill in this section if and Signature person other than parent, make sure that you don't make any mistakes here. The two of these are considered the key ones in this form.
3. Completing Distribution, WhiteCounty, and PinkParentRelativeGuardian is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!

Step 3: Prior to moving on, make sure that all blank fields were filled out right. When you confirm that it's good, press “Done." Make a free trial account with us and get immediate access to Los - which you'll be able to then work with as you wish in your personal account page. Here at FormsPal.com, we do everything we can to make certain that all your details are kept private.