
You may prepare pre without difficulty with the help of our online tool for PDF editing. To make our editor better and less complicated to use, we continuously come up with new features, with our users' feedback in mind. It just takes a few simple steps:
Step 1: Click the "Get Form" button at the top of this page to access our editor.
Step 2: This editor grants the capability to change PDF documents in a range of ways. Modify it by adding any text, correct what's originally in the PDF, and put in a signature - all within the reach of a few clicks!
In an effort to complete this PDF form, ensure that you provide the right details in each and every field:
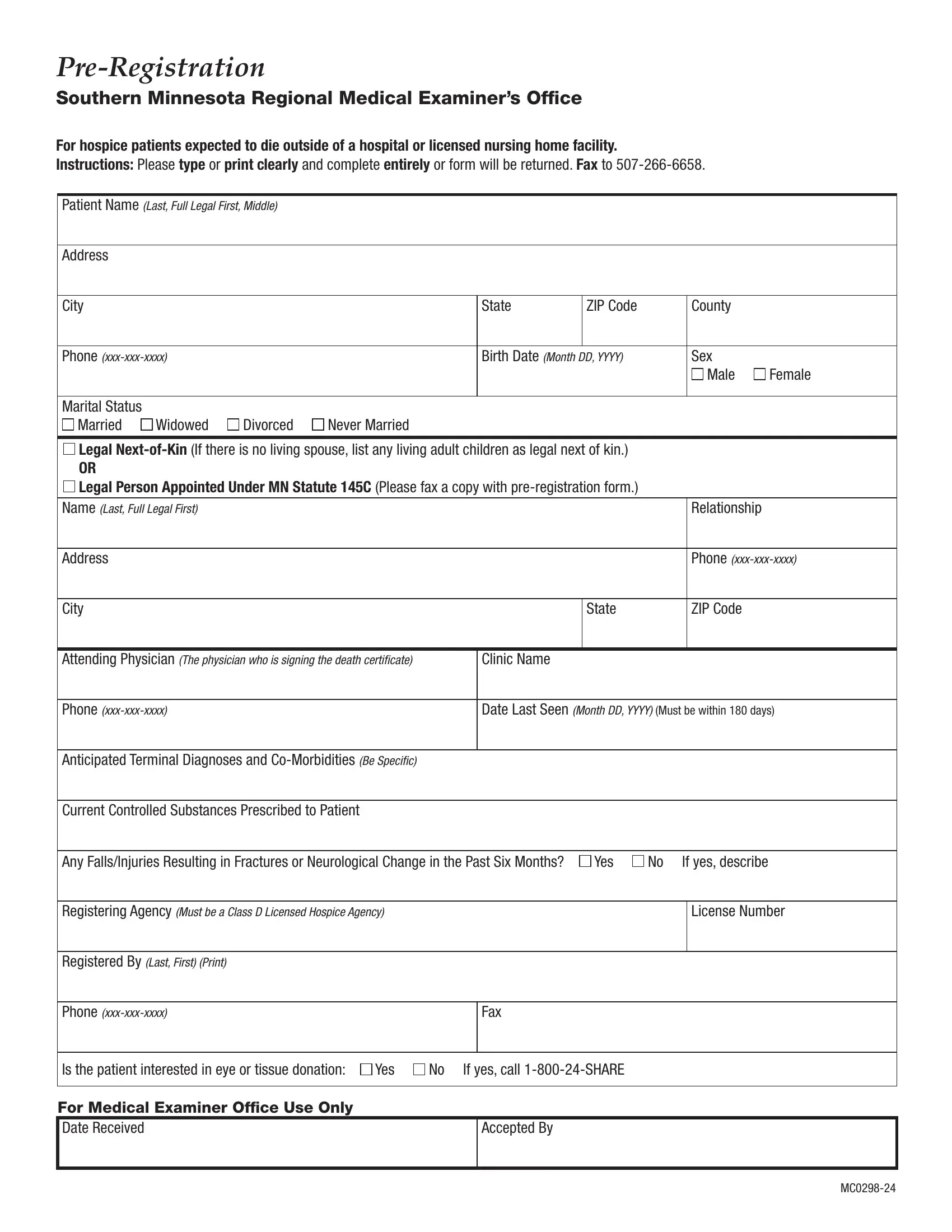
1. Complete the pre with a selection of essential blanks. Get all the important information and be sure there is nothing missed!

2. Once your current task is complete, take the next step – fill out all of these fields - Attending Physician The physician, Clinic Name, Phone xxxxxxxxxx, Date Last Seen Month DD YYYY Must, Anticipated Terminal Diagnoses and, Current Controlled Substances, Any FallsInjuries Resulting in, Yes, No If yes describe, Registering Agency Must be a Class, License Number, Registered By Last First Print, Phone xxxxxxxxxx, Fax, and Is the patient interested in eye with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
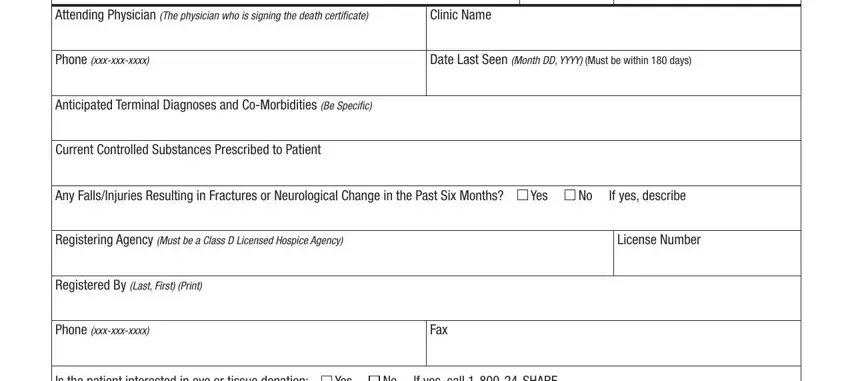
Always be very careful while filling in Registering Agency Must be a Class and Yes, because this is the part where most users make a few mistakes.
Step 3: Revise the information you've typed into the blanks and then click on the "Done" button. Make a free trial option with us and acquire instant access to pre - which you are able to then start using as you wish from your personal account page. We do not share or sell the information that you type in whenever working with documents at FormsPal.