If you're a business owner, you'll want to familiarize yourself with Form Mo 580 0764. This is the Missouri Department of Revenue's form for apportioning income and making adjustments to taxable income. The form can be used by Sole Proprietorships, Partnerships, and Corporations doing business in Missouri. Knowing how to complete this form correctly is essential for ensuring that your business pays the correct amount of taxes. If you need assistance filing Form Mo 580 0764, please contact the Missouri Department of Revenue. Thank you for your time!
| Question | Answer |
|---|---|
| Form Name | Form Mo 580 0764 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | OrderForm missouri department health request form immunology |
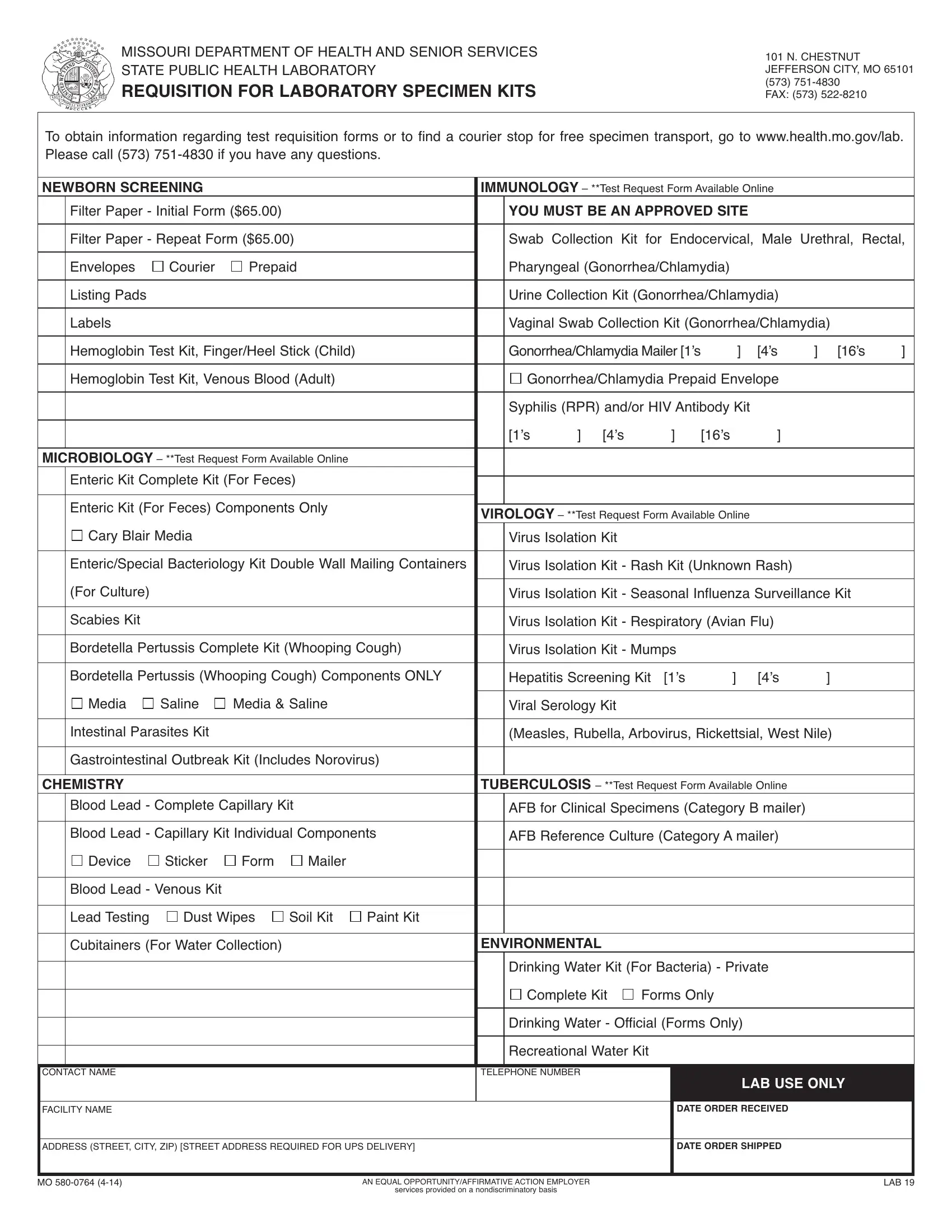
MISSOURI DEPARTMEnT OF HEALTH AnD SEnIOR SERVICES STATE PUBLIC HEALTH LABORATORy
REQUISITION FOR LABORATORY SPECIMEN KITS |
101 n. CHESTnUT JEFFERSOn CITy, MO 65101
(573)
To obtain information regarding test requisition forms or to find a courier stop for free specimen transport, go to www.health.mo.gov/lab. Please call (573)
NEWBORN SCREENING |
|
|
IMMUNOLOGY– **Test Request Form Available Online |
|
|
|||||||
|
Filter Paper - Initial Form ($65.00) |
|
|
YOU MUST BEANAPPROVED SITE |
|
|
|
|||||
|
|
|
|
|||||||||
|
Filter Paper - Repeat Form ($65.00) |
|
Swab Collection Kit for Endocervical, Male Urethral, Rectal, |
|||||||||
|
|
|
|
|
|
|
|
|
||||
|
Envelopes |
Courier |
Prepaid |
|
Pharyngeal (Gonorrhea/Chlamydia) |
|
|
|
||||
|
|
|
|
|
|
|
|
|
||||
|
Listing Pads |
|
|
|
|
Urine Collection Kit (Gonorrhea/Chlamydia) |
|
|
||||
|
|
|
|
|
|
|
|
|||||
|
Labels |
|
|
|
|
Vaginal Swab Collection Kit (Gonorrhea/Chlamydia) |
|
|||||
|
|
|
|
|
|
|
|
|||||
|
Hemoglobin Test Kit, Finger/Heel Stick (Child) |
|
Gonorrhea/ChlamydiaMailer[1’s |
] |
[4’s |
] [16’s |
] |
|||||
|
|
|
|
|
|
|||||||
|
Hemoglobin Test Kit, Venous Blood (Adult) |
|
Gonorrhea/Chlamydia Prepaid Envelope |
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
Syphilis (RPR) and/or HIV Antibody Kit |
|
|
|
|||
|
|
|
|
|
|
[1’s |
] [4’s |
] |
[16’s |
] |
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|||
MICROBIOLOGY– **Test Request Form Available Online |
|
|
|
|
|
|
|
|
||||
|
Enteric Kit Complete Kit (For Feces) |
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|||
|
Enteric Kit (For Feces) Components Only |
|
|
|
|
|
|
|
|
|||
|
VIROLOGY– **Test Request Form Available Online |
|
|
|
||||||||
|
|
|
|
|
|
|
|
|||||
|
Cary Blair Media |
|
|
|
Virus Isolation Kit |
|
|
|
|
|
||
|
|
|
|
|
|
|||||||
|
Enteric/Special Bacteriology Kit Double Wall Mailing Containers |
|
Virus Isolation Kit - Rash Kit (Unknown Rash) |
|
|
|||||||
|
(For Culture) |
|
|
|
|
|
|
|||||
|
|
|
|
|
Virus Isolation Kit - Seasonal Influenza Surveillance Kit |
|
||||||
|
|
|
|
|
|
|
|
|
||||
|
Scabies Kit |
|
|
|
|
Virus Isolation Kit - Respiratory (Avian Flu) |
|
|
||||
|
|
|
|
|
|
|
|
|||||
|
Bordetella Pertussis Complete Kit (Whooping Cough) |
|
Virus Isolation Kit - Mumps |
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
||||
|
Bordetella Pertussis (Whooping Cough) Components OnLy |
|
Hepatitis Screening Kit |
[1’s |
] |
[4’s |
] |
|
||||
|
Media |
Saline |
Media & Saline |
|
|
|
|
|
|
|
||
|
|
Viral Serology Kit |
|
|
|
|
|
|||||
|
|
|
|
|
|
|
||||||
|
Intestinal Parasites Kit |
|
|
|
(Measles, Rubella, Arbovirus, Rickettsial, West nile) |
|
||||||
|
|
|
|
|
|
|
|
|
|
|||
|
Gastrointestinal Outbreak Kit (Includes norovirus) |
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
||||
CHEMISTRY |
|
|
|
TUBERCULOSIS – **Test Request Form Available Online |
|
|
||||||
|
Blood Lead - Complete Capillary Kit |
|
AFB for Clinical Specimens (Category B mailer) |
|
|
|||||||
|
|
|
|
|
|
|||||||
|
Blood Lead - Capillary Kit Individual Components |
|
AFB Reference Culture (Category A mailer) |
|
|
|||||||
|
Device |
Sticker |
Form |
Mailer |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Blood Lead - Venous Kit |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Lead Testing Dust Wipes |
Soil Kit Paint Kit |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|||
|
Cubitainers (For Water Collection) |
|
ENVIRONMENTAL |
|
|
|
|
|
||||
|
|
|
|
|
|
Drinking Water Kit (For Bacteria) - Private |
|
|
||||
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
Complete Kit Forms Only |
|
|
|
|||
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
Drinking Water - Official (Forms Only) |
|
|
|
|||
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Recreational Water Kit |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
COnTACT nAME
TELEPHOnE nUMBER
LAB USE ONLY
FACILITy nAME
DATE ORDER RECEIVED
ADDRESS (STREET, CITy, ZIP) [STREET ADDRESS REQUIRED FOR UPS DELIVERy]
DATE ORDER SHIPPED
MO |
An EQUAL OPPORTUnITy/AFFIRMATIVE ACTIOn EMPLOyER |
LAB 19 |
|
services provided on a nondiscriminatory basis |
|