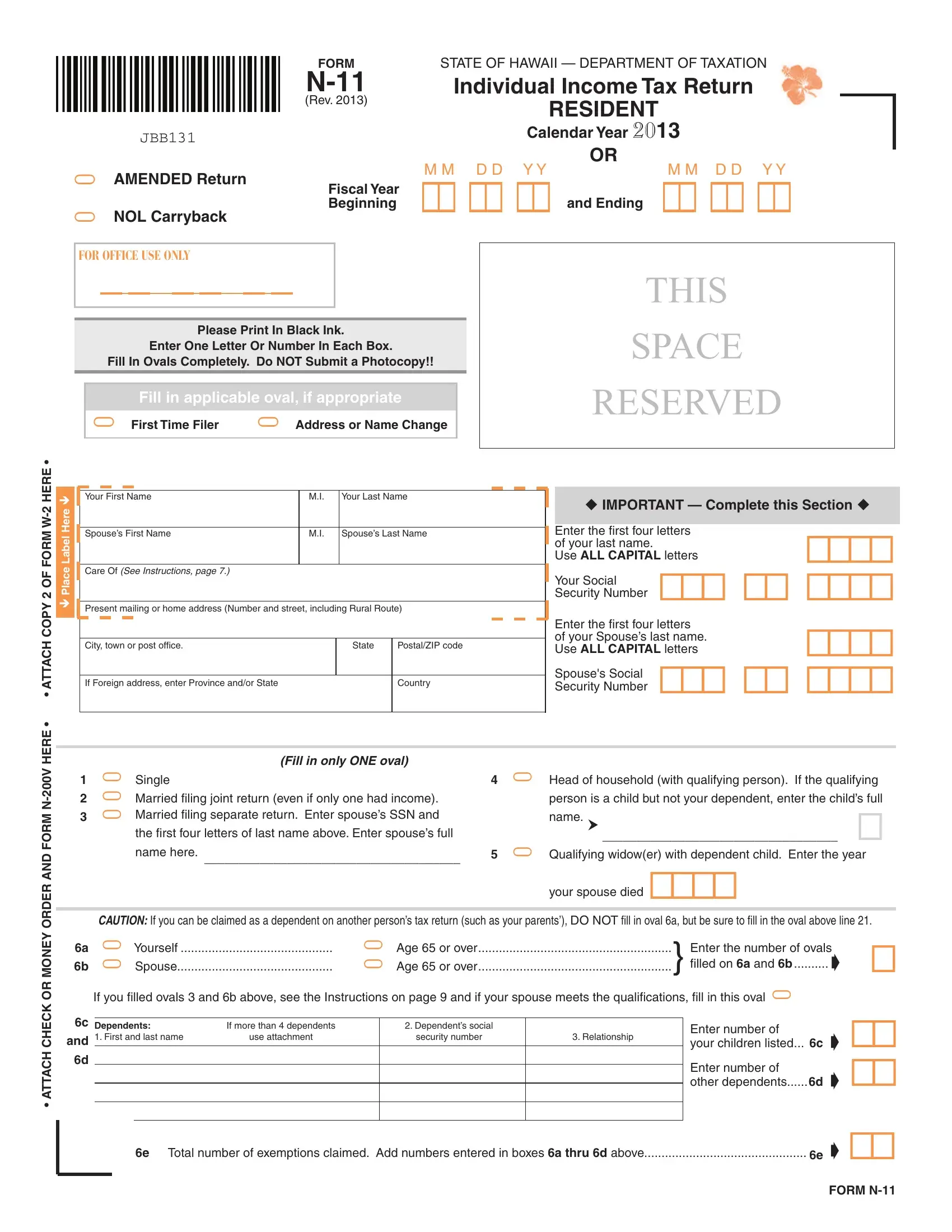
The Form N-11, recognized as the Individual Income Tax Return for residents of Hawaii, plays a crucial role in the financial obligations that accompany each fiscal year. Revised in 2013 for the tax year of that period, this document intricately lays down the procedure for reporting income, calculating taxes owed, or determining refunds due to the taxpayer. With specific sections dedicated to personal information, income details, adjustments, deductions, and credits, it accommodates a comprehensive financial review for individuals operating within the state's jurisdiction. It notably includes provisions for various statuses and situations including—but not limited to—marital status, dependents, special deductions, and tax credits aimed at lessening the fiscal burden on qualifying residents. Designed with precision for office use, the form insists on clarity, advising the use of black ink and cautioning against the submission of photocopies. Additionally, it extends to cover unique financial dynamics such as interest on out-of-state bonds, contributions to exceptional trees, and military or national guard pay adjustments, encapsulating the diverse elements that contribute to an individual's tax responsibility. With meticulous sections for refundable and nonrefundable tax credits along with detailed instructions for amended returns, the Form N-11 encapsulates the State of Hawaii's approach to equitable tax collection and the responsibilities of its residents therein.
| Question | Answer |
|---|---|
| Form Name | Form N 11 |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | form n 11 fillable, hawaii form n 11 fillable, form n 11 rev 2013, hawaii form n 11 |
|
|
|
|
FORM |
STATE OF HAWAII — DEPARTMENT OF TAXATION |
||||||||
|
|
|
|
Individual Income Tax Return |
|
|
|||||||
|
|
|
|
(Rev. 2013) |
|
|
|
|
RESIDENT |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
JBB131 |
|
|
|
Calendar Year 2013 |
|
|||||
|
|
|
|
|
|
|
|
|
|
OR |
|
||
|
|
|
|
|
|
|
|
|
|
|
|||
= AMENDED Return |
M M D D Y Y |
M M D D Y Y |
|||||||||||
!! !! !! |
and Ending !! !! !! |
||||||||||||
|
|
|
|
Fiscal Year |
|||||||||
|
|
|
|
Beginning |
|||||||||
= NOL Carryback |
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
||
FOR OFFICE USE ONLY |
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
THIS |
|||
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
Please Print In Black Ink. |
|
|
|
|
SPACE |
|||||
|
|
|
Enter One Letter Or Number In Each Box. |
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
||||
|
|
Fill In Ovals Completely. Do NOT Submit a Photocopy!! |
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
RESERVED |
|||
|
|
|
Fill in applicable oval, if appropriate |
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|||||
|
= First Time Filer = Address or Name Change |
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
HERE • • ATTACH COPY 2 OF FORM
Place Label Here
Your First Name |
M.I. |
Your Last Name |
|
|
|
Spouse’s First Name |
M.I. |
Spouse’s Last Name |
|
|
|
Care Of (See Instructions, page 7.) |
|
|
Present mailing or home address (Number and street, including Rural Route)
City, town or post office. |
State |
Postal/ZIP code |
|
|
|
If Foreign address, enter Province and/or State |
|
Country |
|
|
|
IMPORTANT — Complete this Section
Enter the first four letters |
!!!! |
Use ALL CAPITAL letters |
|
of your last name. |
|
Your Social !!! !! !!!!
Security Number
Enter the first four letters
of your Spouse’s last name.!!!!
Use ALL CAPITAL letters
Spouse's Social !!! !! !!!!
Security Number
• ATTACH CHECK OR MONEY ORDER AND FORM
|
|
(Fill in only ONE oval) |
|
|
|
1 |
= Single |
|
4 |
= Head of household (with qualifying person). If the qualifying |
|
2 |
= Married filing joint return (even if only one had income). |
|
person is a child but not your dependent, enter the child’s full |
||
3 |
= Married filing separate return. Enter spouse’s SSN and |
|
name. h __________________________________ |
! |
|
the first four letters of last name above. Enter spouse’s full |
|
||||
|
name here. |
_____________________________________ |
5 |
= Qualifying widow(er) with dependent child. Enter the year |
|
|
|
|
|
|
|
your spouse died !!!!
CAUTION: If you can be claimed as a dependent on another person’s tax return (such as your parents’), DO NOT fill in oval 6a, but be sure to fill in the oval above line 21.
6a |
= Yourself |
= Age 65 or over |
} |
Enter the number of ovals |
! |
||||||
6b |
= Spouse |
= Age 65 or over |
filled on 6a and 6b |
.......... |
¶ |
||||||
|
If you filled ovals 3 and 6b above, see the Instructions on page 9 and if your spouse meets the qualifications, fill in this oval = |
|
|
|
|||||||
6c |
|
|
|
|
|
|
|
|
|
|
!! |
Dependents: |
If more than 4 dependents |
|
2. Dependent’s social |
|
|
Enter number of |
|
¶ |
|||
and |
1. First and last name |
use attachment |
|
security number |
3. Relationship |
|
your children listed |
... 6c |
|||
|
|
|
|
|
|
|
|||||
6d |
|
|
|
|
|
|
|
Enter number of |
|
|
!! |
|
|
|
|
|
|
|
|
|
¶ |
||
|
|
|
|
|
|
|
|
other dependents |
6d |
||
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6e Total number of exemptions claimed. Add numbers entered in boxes 6a thru 6d above |
6e ¶ !! |
FORM
|
Form |
Page 2 of 4 |
|
|
Your Social Security Number |
Your Spouse’s SSN |
|
JBB132 |
!!! !! !!!! |
!!! !! !!!! |
|
|
|
|
|
Name(s) as shown on return ___________________________________________________
If amount is negative (loss), shade the minus
|
|
|
|
|
|
ROUND TO THE NEAREST DOLLAR |
|||
|
|
|
7 |
|
!!!,!!!,!!!.00 |
||||
7 |
Federal adjusted gross income (AGI) (see page 11 of the Instructions) |
- |
|||||||
|
|||||||||
8 |
Difference in state/federal wages due to COLA, ERS, |
|
!!!,!!!,!!!.00 |
|
|
||||
|
|
|
|
|
|
||||
|
etc. (see page 11 of the Instructions) |
8 |
!!!,!!!,!!!.00 |
|
|
||||
9 |
Interest on |
|
|
|
|
||||
|
|
|
|
|
|
|
|||
|
(including municipal bonds) |
9 |
!!!,!!!,!!!.00 |
|
|
||||
10 |
Other Hawaii additions to federal AGI |
|
|
|
|||||
|
|
|
|
|
|
||||
|
(see page 11 of the Instructions) |
10 |
|
|
!!!,!!!,!!!.00 |
||||
11 |
Add lines 8 through 10 |
Total Hawaii additions to federal AGI |
11 |
||||||
|
|
|
|||||||
|
|
|
|
|
|
12 |
|
!!!,!!!,!!!.00 |
|
12 |
Add lines 7 and 11 |
|
|
|
- |
||||
|
|
|
|
||||||
13 |
Pensions taxed federally but not taxed by Hawaii |
13 |
!!!,!!!,!!!.00 |
|
|
||||
14 |
Social security benefits taxed on federal return |
14 |
!!!,!!!,!!!.00 |
|
|
||||
!!!,!!!,!!!.00 |
|
|
|||||||
15 |
First $6,076 of military reserve or Hawaii national |
|
|
|
|||||
|
|
|
|
|
|
||||
|
guard duty pay |
15 |
!!!,!!!,!!!.00 |
|
|
||||
16 |
Payments to an individual housing account |
16 |
|
|
|||||
!!!,!!!,!!!.00 |
|
|
|||||||
17 |
Exceptional trees deduction (attach affidavit) |
|
|
|
|||||
|
|
|
|
|
|
||||
|
(see page 14 of the Instructions) |
17 |
!!!,!!!,!!!.00 |
|
|
||||
18 |
Other Hawaii subtractions from federal AGI |
|
|
|
|||||
|
|
|
|
|
|
||||
|
(see page 14 of the Instructions) |
18 |
|
|
!!!,!!!,!!!.00 |
||||
19 |
Add lines 13 through 18 |
|
|
|
|
||||
|
|
|
|
|
|
|
|||
|
............................................ Total Hawaii subtractions from federal AGI |
19 |
|
|
|
||||
|
|
|
|
|
Hawaii AGI ³ 20 |
|
!!!,!!!,!!!.00 |
||
20 |
Line 12 minus line 19 |
|
|
- |
|||||
|
|
|
|||||||
CAUTION: If you can be claimed as a dependent on another person’s return, see the Instructions on page 16, and fill in this oval. =
21If you do not itemize your deductions, go to line 23 below. Otherwise go to page 16 of the Instructions and enter your itemized deductions here.
21a Medical and dental expenses |
|
(from Worksheet |
21a |
21b |
Taxes (from Worksheet |
21b |
21c |
Interest expense (from Worksheet |
21c |
21d |
Contributions (from Worksheet |
21d |
21e |
Casualty and theft losses (from Worksheet |
21e |
21f |
Miscellaneous deductions (from Worksheet |
21f |
23If you checked filing status box: 1 or 3 enter $2,200;
2 or 5 enter $4,400; 4 enter $3,212 |
Standard Deduction ³ 23 |
|
24 Line 20 minus line 22 or 23, whichever applies. (This line MUST be filled in) |
24 |
|
TOTAL ITEMIZED
DEDUCTIONS
22Add lines 21a through 21f. If your adjusted gross income is above a certain amount, you may not be able to deduct all of your itemized deductions. See the Instructions on page 21. Enter total here and go to line 24.
!!!,!!!,!!!.00
!!!,!!!,!!!.00
-!!!,!!!,!!!.00
FORM
|
Form |
Page 3 of 4 |
|
|
Your Social Security Number |
Your Spouse’s SSN |
|
JBB133 |
!!! !! !!!! |
!!! !! !!!! |
|
|
|
|
|
Name(s) as shown on return ___________________________________________________
25If line 20 is $89,981 or less, multiply $1,144 by the total number of exemptions claimed on line 6e. Otherwise, see page 22 of the Instructions. If you and/or your spouse are blind, deaf, or disabled, fill in the applicable oval(s), and see page 22 of the Instructions.
|
= Yourself |
= Spouse |
|
25 |
|
26 |
Taxable Income. Line 24 minus line 25 (but not less than zero) |
................... |
Taxable Income ³ 26 |
||
27 |
Tax. Fill in oval if from = Tax Table; = Tax Rate Schedule; or |
= Capital Gains Tax |
|||
|
Worksheet on page 39 of the Instructions. |
|
|
|
|
|
( = Fill in oval if tax from Forms |
||||
|
|
Tax ³ 27 |
|||
27a |
If tax is from the Capital Gains Tax Worksheet, enter |
|
|
|
|
|
the net capital gain from line 14 of that worksheet |
27a |
|
|
|
|
|
|
|
!!!,!!!,!!!.00 |
|
!!!,!!!,!!!.00
!!!,!!!,!!!.00
!!!,!!!,!!!.00
28 |
Refundable Food/Excise Tax Credit |
!! |
|
|
(attach Schedule X) DHS, etc. exemptions |
.... 28 |
|
29 |
Credit for |
|
|
|
Renters (attach Schedule X) |
29 |
|
30 |
Credit for Child and Dependent |
|
|
|
Care Expenses (attach Schedule X) |
30 |
|
31 |
Credit for Child Passenger Restraint |
|
|
|
System(s) (attach a copy of the invoice) |
31 |
|
32 |
Total refundable tax credits from |
|
|
|
Schedule CR (attach Schedule CR) |
32 |
|
33 |
Add lines 28 through 32 |
Total Refundable Credits ³ 33 |
|
34 |
Line 27 minus line 33. If line 34 is zero or less, see Instructions. |
.................................................. 34 |
|
35 |
Total nonrefundable tax credits (attach Schedule CR) |
35 |
|
36 |
Line 34 minus line 35 |
Balance ³ 36 |
|
37 |
Hawaii State Income tax withheld (attach |
|
!!!,!!!,!!!.00 |
|
(see page 27 of the Instructions for other attachments) |
37 |
|
|
|
|
|
38 |
2013 estimated tax payments |
38 |
!!!,!!!,!!!.00 |
|
|
|
|
39 |
Amount of estimated tax applied from 2012 return |
39 |
!!!,!!!,!!!.00 |
|
|
|
|
40 |
Amount paid with extension |
40 |
!!!,!!!,!!!.00 |
|
|
|
|
!!!,!!!,!!!.00
-!!!,!!!,!!!.00
!!!,!!!,!!!.00
-!!!,!!!,!!!.00
41 Add lines 37 through 40 |
Total Payments ³ 41 |
!!!,!!!,!!!.00 |
|
42 |
If line 41 is larger than line 36, enter the amount OVERPAID (line 41 minus line 36) (see Instructions).. 42 |
||
43 |
Contributions to (see page 28 of the Instructions): |
Yourself |
Spouse |
|
43a Hawaii Schools Repairs and Maintenance Fund |
= $2 |
= $2 |
|
43b Hawaii Public Libraries Fund |
= $2 |
= $2 |
|
43c Domestic and Sexual Violence / Child Abuse and Neglect Funds |
= $5 |
= $5 |
44 |
Add the amounts of the filled ovals on lines 43a through 43c and enter the total here |
................. 44 |
|
|
45 Line 42 minus line 44 |
45 |
|
!!!,!!!,!!!.00
!!.00
!!!,!!!,!!!.00
FORM
|
Form |
|
|
Page 4 of 4 |
||
|
Your Social Security Number |
Your Spouse’s SSN |
||||
JBB134 |
!!! !! !!!! |
!!! !! !!!! |
|
|
||
|
|
|
|
|
|
|
|
Name(s) as shown on return ___________________________________________________ |
|
||||
|
|
|||||
46 Amount of line 45 to be applied to your |
|
!!!,!!!,!!!.00 |
|
|
|
|
|
|
|
|
|
|
|
2014 ESTIMATED TAX |
46 |
|
|
!!!,!!!,!!!.00 |
|
|
47a Amount to be REFUNDED TO YOU (line 45 minus line 46) If filing late, |
|
|
||||
|
|
|
|
|||
see page 28 of Instructions |
|
47a |
|
|
|
|
=Fill in this oval if this refund will ultimately be deposited to a foreign
b |
Routing number |
!!!!!!!!! |
c Type: = Checking |
= Savings |
|
|
d |
Account number |
!!!!!!!!!!!!!!!!! |
|
|
||
48 |
AMOUNT YOU OWE (line 36 minus line 41). Send Form |
|
!!!,!!!,!!!.00 |
|||
|
Make check or money order payable to the “Hawaii State Tax Collector” |
48 |
||||
49 |
Estimated tax penalty. (See page 29 of |
|
|
|
||
|
|
|
|
|||
|
Instructions.) Do not include on line 42 or 48. Fill in |
|
!!!,!!!,!!!.00 |
|
||
|
this oval if Form |
49 |
|
|||
|
|
|
|
|
||
50 |
AMENDED RETURN ONLY – |
Amount paid (overpaid) on original return. (See Instructions) (attach Sch. AMD) |
50 |
51 |
AMENDED RETURN ONLY – |
Balance due (refund) with amended return. (See Instructions) (attach Sch. AMD) |
51 |
-!!!,!!!,!!!.00
-!!!,!!!,!!!.00
52 |
Did you file a federal Schedule C? |
= Yes |
= No |
If yes, enter Hawaii gross receipts |
!!!,!!!,!!!.00 |
|||
|
your main business activity: |
|
|
|
, |
|
||
|
|
AND your HI Tax I.D. No. for this activity W !!!!!!!! — !! |
||||||
|
your main business product: |
|
|
|
, |
|||
|
|
|
|
|||||
53 |
Did you file a federal Schedule E |
|
|
|
If yes, enter Hawaii gross rents received |
!!!,!!!,!!!.00 |
||
|
for any rental activity? |
= Yes |
= No |
|
||||
|
AND your HI Tax I.D. No. for this activity W !!!!!!!! — !! |
|||||||
|
|
|
|
|
|
|
||
54 |
Did you file a federal Schedule F? |
= Yes |
= No |
If yes, enter Hawaii gross receipts |
!!!,!!!,!!!.00 |
|||
|
your main business activity: |
|
|
|
, |
|
||
|
|
AND your HI Tax I.D. No. for this activity W !!!!!!!! — !! |
||||||
|
your main business product: |
|
|
|
, |
|||
|
|
|
|
|||||
DESIGNEE
If designating another person to discuss this return with the Hawaii Department of Taxation, complete the following. This is not a full power of attorney. See page 30 of the Instructions.
Designee’s name h |
Phone no. h |
Identification number h |
HAWAII ELECTION CAMPAIGN FUND
Do you want $3 to go to the Hawaii Election Campaign Fund? |
= |
Yes |
= |
No |
If joint return, does your spouse want $3 to go to the fund? |
= |
Yes |
= |
No |
|
|
|
|
|
Note: Filling in the “Yes” oval will not increase your tax or reduce your refund.
PLEASE SIGN HERE
DECLARATION — I declare, under the penalties set forth in section
|
Your signature |
|
|
Date |
|
|
Spouse’s signature (if filing jointly, BOTH must sign) |
Date |
||||
|
|
|
||||||||||
h |
|
|
|
|
|
h |
|
|
|
|
||
|
Your Occupation |
|
|
Daytime Phone Number |
|
|
Your Spouse’s Occupation |
|
|
Daytime Phone Number |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Preparer’s |
h |
|
|
|
|
Date |
Check if |
|
Preparer’s identification number |
|
|
|
|
|
|
|
|
h |
|
|
|||
|
|
Signature |
|
|
|
|
|
|
|
|||
Paid |
|
|
|
|
|
|
|
|
|
|
|
|
|
h |
|
|
|
|
|
|
|
|
|||
Preparer’s |
|
|
|
|
|
Federal E.I. No. h |
|
|||||
Preparer’s Name |
|
|
|
|
|
|||||||
Information |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Firm’s name (or yours |
|
|
|
|
Phone No. h |
|
||||
|
|
if |
h |
|
|
|
|
|
||||
|
|
Address, and ZIP Code |
|
|
|
|
|
|
|
|
||
FORM