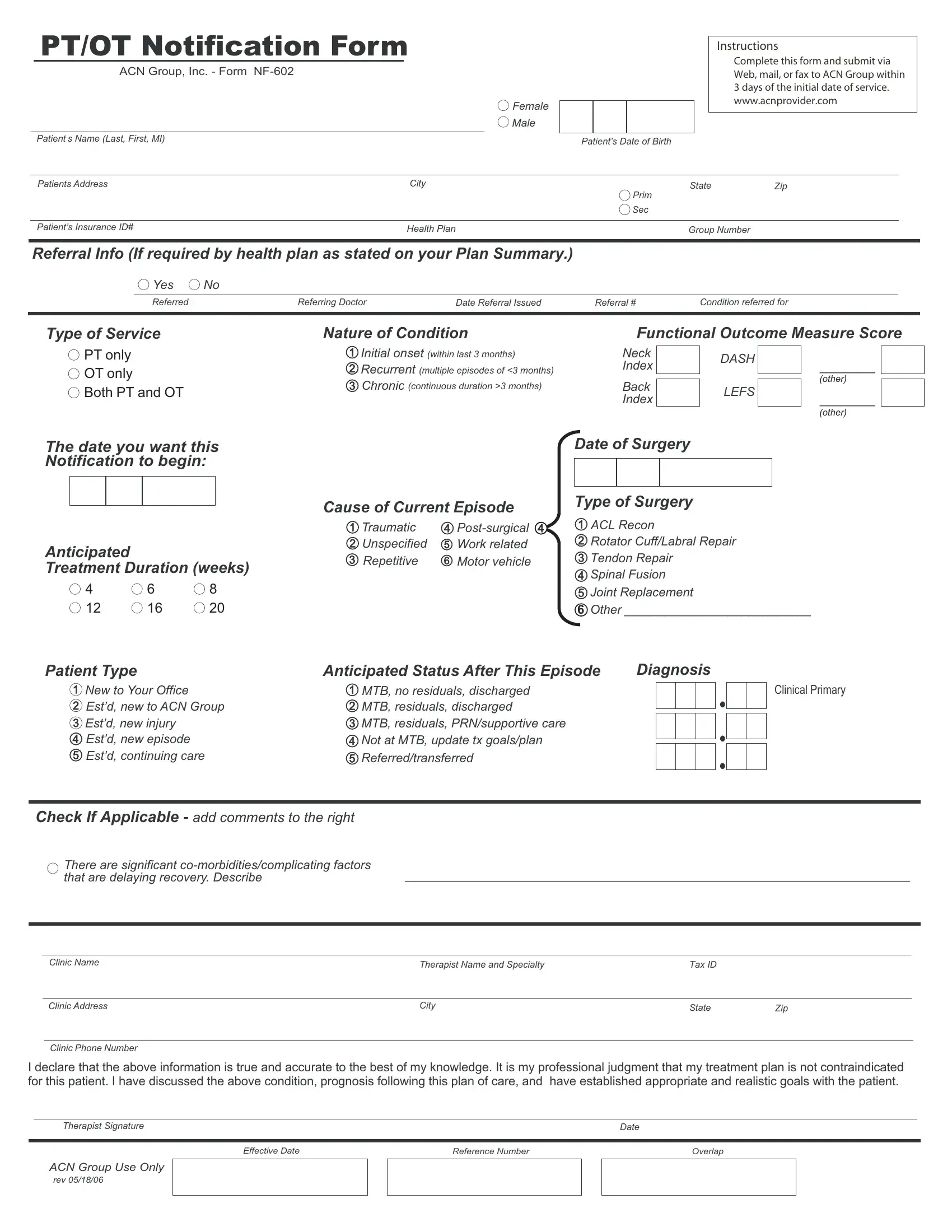
The NF-602 form serves as a crucial notification tool within the healthcare sector, specifically tailored for physical therapy (PT) and occupational therapy (OT) services. This comprehensive document, administered by ACN Group, Inc., requires health professionals to provide detailed information about patients undergoing therapy. From basic patient identifiers like name, date of birth, and insurance details to intricate elements covering referral information, type of service needed, and the nature of the condition, the form spans several critical data points. It mandates therapists to report on the functional outcome measure score, condition onset, and anticipated treatment duration, encompassing options from 4 to 20 weeks. Furthermore, the form delves into specifics surrounding the patient's episode, including the cause, type of surgery if applicable, and anticipated status post-treatment. Therapists must also note any significant co-morbidities that could impede recovery, ensuring a comprehensive view of the patient's health is considered. By signing the NF-602, therapists affirm the accuracy of the information and the tailored treatment plan's appropriateness for the patient. This crucial step aids in streamlining care coordination and ensuring that both new and established patients within the ACN Group network receive timely and effective therapy services.
| Question | Answer |
|---|---|
| Form Name | Form Nf 602 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | morbidities, tx, contraindicated, uhc acn form |

PT/OT NOTIFICATION FORM
ACN Group, Inc. - Form
|
Female |
|
|
|
|
Male |
|
|
|
|
|
|
|
|
Patient s Name (Last, First, MI) |
|
Patient’s Date of Birth |
||
|
|
|||
Instructions
Complete this form and submit via Web, mail, or fax to ACN Group within 3 days of the initial date of service. www.acnprovider.com
|
Patients Address |
City |
State |
Zip |
|
|
|
|
|
||
|
|
|
Prim |
|
|
|
|
|
Sec |
|
|
|
|
|
|
|
|
|
Patient’s Insurance ID# |
Health Plan |
Group Number |
|
|
|
|
|
|
|
|
Referral Info (If required by health plan as stated on your Plan Summary.)
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
Referred |
Referring Doctor |
Date Referral Issued |
Referral # |
Condition referred for |
|
|
|
|
|
|
|
|
Type of Service |
Nature of Condition |
|
Functional Outcome Measure Score |
|||
PT only |
Initial onset (within last 3 months) |
Neck |
OT only |
Recurrent (multiple episodes of <3 months) |
Index |
|
||
Chronic (continuous duration >3 months) |
|
|
Both PT and OT |
Back |
|
|
Index |
|
|
|
DASH
LEFS
________
(other)
________
(other)
The date you want this Notification to begin:
Anticipated
Treatment Duration (weeks)
4 |
6 |
8 |
12 |
16 |
20 |
Patient Type
New to Your Office
Est’d, new to ACN Group
Est’d, new injury
Est’d, new episode Est’d, continuing care
|
|
Date of Surgery |
Cause of Current Episode |
Type of Surgery |
|
|
||
Traumatic |
ACL Recon |
|
Unspecified |
Work related |
Rotator Cuff/Labral Repair |
Repetitive |
Motor vehicle |
Tendon Repair |
|
||
Spinal Fusion
Joint Replacement
6Other ___________________________
Anticipated Status After This Episode |
Diagnosis |
. |
|
MTB, no residuals, discharged |
|
Clinical Primary |
|
MTB, residuals, discharged |
|
. |
|
MTB, residuals, PRN/supportive care |
|
|
|
|
|
|
|
Not at MTB, update tx goals/plan |
|
. |
|
Referred/transferred |
|
|
Check If Applicable - add comments to the right
There are significant
Clinic Name |
Therapist Name and Specialty |
Tax ID |
|
|
|
|
|
Clinic Address |
City |
State |
Zip |
|
|
Clinic Phone Number
I declare that the above information is true and accurate to the best of my knowledge. It is my professional judgment that my treatment plan is not contraindicated for this patient. I have discussed the above condition, prognosis following this plan of care, and have established appropriate and realistic goals with the patient.
Therapist Signature |
|
Date |
|
|
|
Effective Date |
Reference Number |
Overlap |
ACN Group Use Only
rev 05/18/06