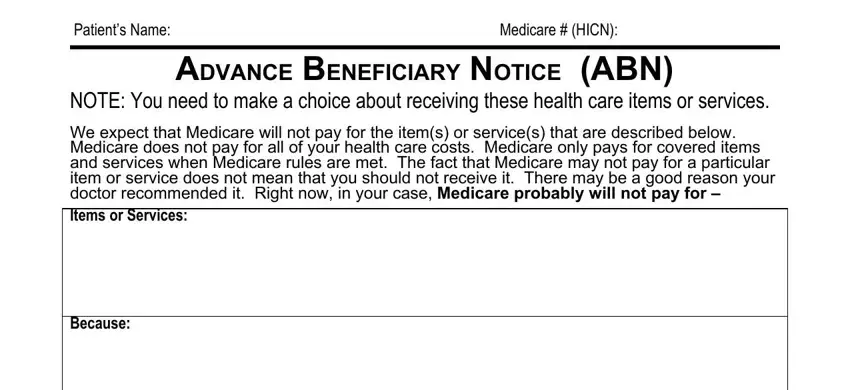
Patient’s Name: |
Medicare # (HICN): |
|
|
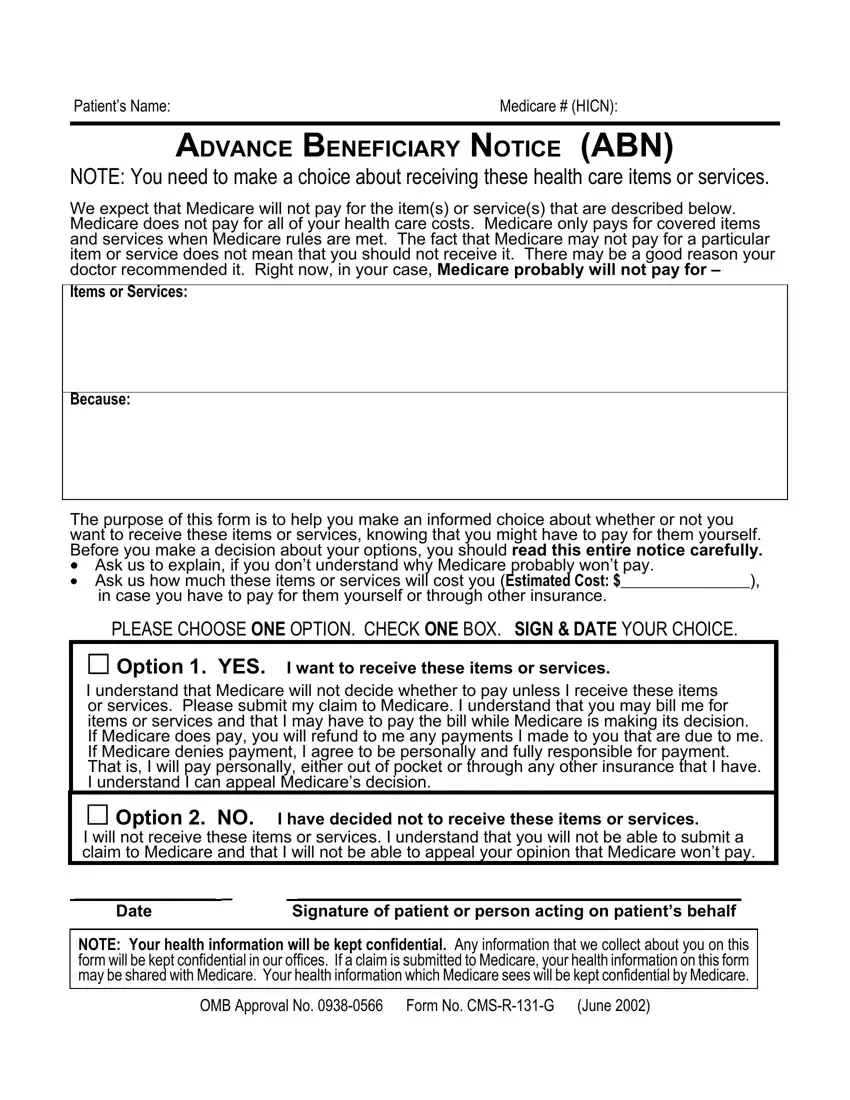
ADVANCE BENEFICIARY NOTICE (ABN)
NOTE: You need to make a choice about receiving these health care items or services.
We expect that Medicare will not pay for the item(s) or service(s) that are described below. Medicare does not pay for all of your health care costs. Medicare only pays for covered items and services when Medicare rules are met. The fact that Medicare may not pay for a particular item or service does not mean that you should not receive it. There may be a good reason your doctor recommended it. Right now, in your case, Medicare probably will not pay for –
Items or Services:
Because:
The purpose of this form is to help you make an informed choice about whether or not you want to receive these items or services, knowing that you might have to pay for them yourself. Before you make a decision about your options, you should read this entire notice carefully.
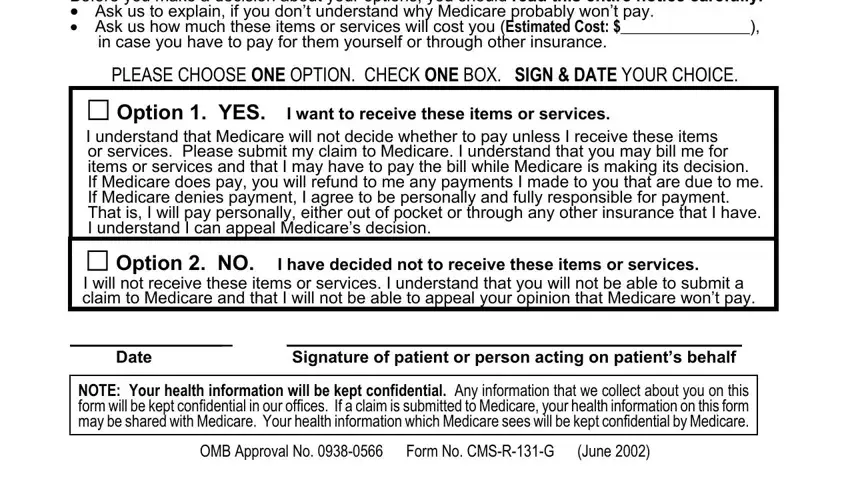
•Ask us to explain, if you don’t understand why Medicare probably won’t pay.
•Ask us how much these items or services will cost you (Estimated Cost: $_________________),
in case you have to pay for them yourself or through other insurance.
PLEASE CHOOSE ONE OPTION. CHECK ONE BOX. SIGN & DATE YOUR CHOICE.
Option 1. YES. I want to receive these items or services.
I understand that Medicare will not decide whether to pay unless I receive these items or services. Please submit my claim to Medicare. I understand that you may bill me for items or services and that I may have to pay the bill while Medicare is making its decision.
If Medicare does pay, you will refund to me any payments I made to you that are due to me. If Medicare denies payment, I agree to be personally and fully responsible for payment. That is, I will pay personally, either out of pocket or through any other insurance that I have. I understand I can appeal Medicare’s decision.
Option 2. NO. I have decided not to receive these items or services.
I will not receive these items or services. I understand that you will not be able to submit a claim to Medicare and that I will not be able to appeal your opinion that Medicare won’t pay.
_____________ _ |
_________________________________________ |
Date |
Signature of patient or person acting on patient’s behalf |
NOTE: Your health information will be kept confidential. Any information that we collect about you on this form will be kept confidential in our offices. If a claim is submitted to Medicare, your health information on this form may be shared with Medicare. Your health information which Medicare sees will be kept confidential by Medicare.
OMB Approval No. 0938-0566 Form No. CMS-R-131-G (June 2002)