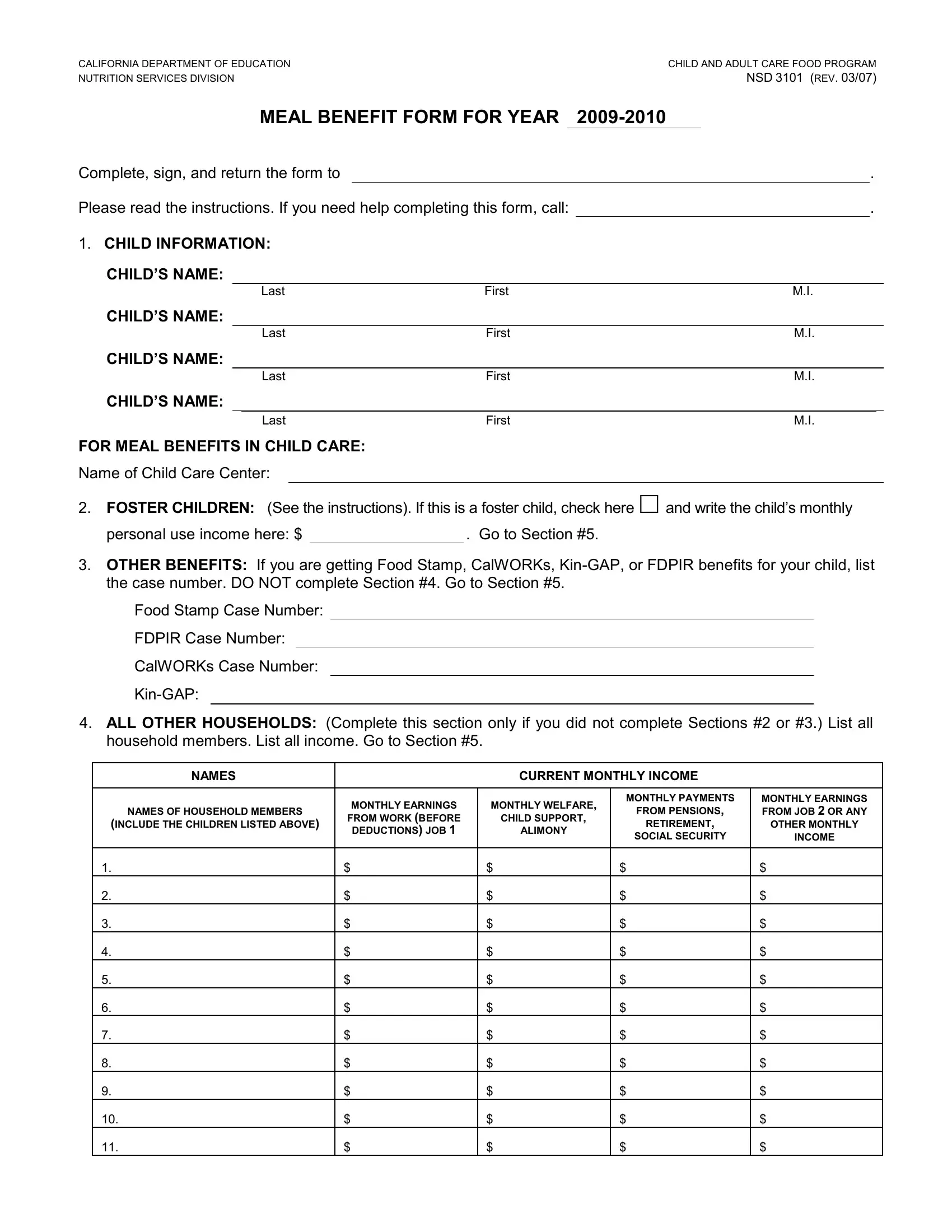
In the efforts to ensure equitable access to meal benefits under the Child and Adult Care Food Program (CACFP), the California Department of Education's Nutrition Services Division provides the NSD 3101 form, a crucial document for the fiscal year 2009-2010. This form, revised in March 2007, serves as a comprehensive application designed to accurately assess and grant meal benefits for children within various care settings. Essential components of the form include sections dedicated to child information, where the names and details of children applying for benefits are listed; specific directions for foster children that streamline their approval process; provisions for households receiving benefits such as Food Stamps, CalWORKs, Kin-GAP, or FDPIR by only requiring case numbers; and a detailed income reporting section for all other households. The form sternly necessitates honest reporting of household income and the signature of an adult household member, underlined by warnings of penalties for misrepresentation, highlighting the importance of integrity in the process. Additionally, it touches on privacy concerns with respect to the provision of Social Security numbers and lays out the procedure for their use in verification processes. The form also inclusively asks for voluntary racial/ethnic identity information, reinforcing the program's commitment to nondiscrimination in accordance with Federal law and U.S. Department of Agriculture policy. Lastly, for thorough guidance, the form concludes with instructions on its completion, ensuring applicants are well-informed on how to proceed accurately, thereby facilitating a smoother review and decision-making process by the CDE officials.
| Question | Answer |
|---|---|
| Form Name | Form Nsd 3101 |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | nsd 3101 cacfp 29 rev 8 2018 in spanish, nsd 3101, nsd3101, USDA |
CALIFORNIA DEPARTMENT OF EDUCATION |
|
|
CHILD AND ADULT CARE FOOD PROGRAM |
|||
NUTRITION SERVICES DIVISION |
|
|
|
NSD 3101 (REV. 03/07) |
||
|
MEAL BENEFIT FORM FOR YEAR |
|
|
|
||
Complete, sign, and return the form to |
|
|
|
. |
||
Please read the instructions. If you need help completing this form, call: |
. |
|||||
1. CHILD INFORMATION: |
|
|
|
|
|
|
CHILD’S NAME: |
|
|
|
|
|
|
|
Last |
First |
|
M.I. |
||
CHILD’S NAME: |
|
|
|
|
|
|
|
Last |
First |
|
M.I. |
||
CHILD’S NAME: |
|
|
|
|
|
|
|
Last |
First |
|
M.I. |
||
CHILD’S NAME: |
|
|
|
|
|
|
|
Last |
First |
|
M.I. |
||
FOR MEAL BENEFITS IN CHILD CARE:
Name of Child Care Center:
2. FOSTER CHILDREN: (See the instructions). If this is a foster child, check here and write the child’s monthly
personal use income here: $ |
|
. Go to Section #5. |
3.OTHER BENEFITS: If you are getting Food Stamp, CalWORKs,
Food Stamp Case Number:
FDPIR Case Number:
CalWORKs Case Number:
4.ALL OTHER HOUSEHOLDS: (Complete this section only if you did not complete Sections #2 or #3.) List all household members. List all income. Go to Section #5.
NAMES |
|
|
CURRENT MONTHLY INCOME |
|
||
|
|
|
|
|
|
|
|
MONTHLY EARNINGS |
MONTHLY WELFARE, |
MONTHLY PAYMENTS |
MONTHLY EARNINGS |
||
NAMES OF HOUSEHOLD MEMBERS |
FROM PENSIONS, |
FROM JOB 2 OR ANY |
||||
FROM WORK (BEFORE |
|
CHILD SUPPORT, |
||||
(INCLUDE THE CHILDREN LISTED ABOVE) |
|
RETIREMENT, |
OTHER MONTHLY |
|||
DEDUCTIONS) JOB 1 |
|
ALIMONY |
||||
|
|
SOCIAL SECURITY |
INCOME |
|||
|
|
|
|
|||
|
|
|
|
|
|
|
1. |
$ |
$ |
|
$ |
$ |
|
2. |
$ |
$ |
|
$ |
$ |
|
3. |
$ |
$ |
|
$ |
$ |
|
4. |
$ |
$ |
|
$ |
$ |
|
5. |
$ |
$ |
|
$ |
$ |
|
6. |
$ |
$ |
|
$ |
$ |
|
7. |
$ |
$ |
|
$ |
$ |
|
8. |
$ |
$ |
|
$ |
$ |
|
9. |
$ |
$ |
|
$ |
$ |
|
10. |
$ |
$ |
|
$ |
$ |
|
11. |
$ |
$ |
|
$ |
$ |
|

CALIFORNIA DEPARTMENT OF EDUCATION |
CHILD AND ADULT CARE FOOD PROGRAM |
NUTRITION SERVICES DIVISION |
NSD 3101 PAGE 2 (REV. 03/07) |
5.SIGNATURE AND SOCIAL SECURITY NUMBER:
PENALTIES FOR MISREPRESENTATION: I certify that all of the above information is true and correct and that the Food Stamp, CalWORKs,
Signature of Adult:
|
|
|
|
|
|
|
|
|
|
|
|
Check here if no |
Social Security Number: |
|
|
|
|
Social Security Number |
|||||||
Printed Name: |
|
|
|
|
|
|
|
|||||
Home Phone: |
|
|
Work Phone: |
|
|
|||||||
Home Address: |
|
|
|
|
|
|
|
|||||
City: |
|
|
|
State: |
|
Zip Code: |
|
|||||
Date: |
|
|
|
|
|
|
|
|||||
Privacy Act Statement: Unless you list the child's Food Stamp, CalWORKs,
the household member signing the form, or indicate that the household member signing the form does not have a social security number. You do not have to list a social security number, but if a social security number is not listed, or the “Check here if no Social Security Number” is not marked, we cannot approve the form. The social security number may be used to identify the household member in verifying the correctness of the information stated on the form. This may include program
reviews, audits and investigations, and may include contacting employers to determine income, contacting a Food Stamp, CalWORKs,
6.RACIAL/ETHNIC IDENTITY: You are not required to answer these questions. If you choose to do so, please mark one or more of the following racial identities:
American Indian or Alaska Native |
Asian |
Black or African American |
Native Hawaiian or Other Pacific Islander |
White |
|
Please mark one of the following ethnic identities: |
Hispanic or Latino |
Not Hispanic or Latino |
In accordance with Federal law and U.S. Department of Agriculture policy, this agency is prohibited from discriminating on the basis of race, color, national origin, sex, age, or disability.
To file a complaint of discrimination, write USDA, Director, Office of Civil Rights, Room
For Official Use Only: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
Yes |
No |
|
For CDE Only |
|
||||
|
|
|
|
|
|
|
|
|||||
Food |
|
|
|
|||||||||
MONTHLY INCOME CONVERSION: WEEKLY X 4.33, EVERY 2 WEEKS X 2.15, TWICE A MONTH X 2 |
|
|
|
|||||||||
|
|
|
|
|||||||||
Total monthly income: |
____________ |
Household size: ________ |
|
|
|
|
|
|
|
|||
Eligibility Classification: |
Free |
Reduced Price |
|
Paid |
|
|
|
|
|
|
||
Determining official (print name): |
|
|
|
|
|
|
|
|
|
|
||
Signature: |
|
|
|
|
|
Date: |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
CALIFORNIA DEPARTMENT OF EDUCATION |
CHILD AND ADULT CARE FOOD PROGRAM |
NUTRITION SERVICES DIVISION |
NSD 3101 PAGE 3 (REV. 03/07) |
HOW TO COMPLETE THE MEAL BENEFIT FORM
Please complete the Meal Benefit Form using the instructions below. Sign the form and return it to:
. If you need help, call:
1.CHILD INFORMATION:
a)Print your child’s name.
B) INCLUDE THE NAME OF THE CHILD CARE CENTER.
2.FOSTER CHILDREN: Complete this Section and sign the form in #5.
a)Write the foster child’s monthly “personal use” income. Write “0” if the foster child does not get “personal use” income.
b)A foster parent or other official representing the child must sign the form in #5. You do not have to list a Social Security Number.
c)Complete a separate form for each foster child.
3.OTHER BENEFITS: Complete this Section and sign the form in #5.
a)List your current Food Stamp, CalWORKs,
b)Sign the form in #5. An adult household member must sign. You do not have to list a Social Security Number.
4.ALL OTHER HOUSEHOLDS: Complete this Section and sign the form in #5.
a)Write the names of everyone in your household even if they do not have an income. Include yourself, your spouse, the child you are applying for, and all other household members.
b)Write the amount of income each person received last month before taxes or anything else was taken out and where it came from, such as earnings, welfare, pensions, and other income (see examples below for types of income to
report). Each income amount should be entered in the appropriate column on the form. If any amount last month was more or less than usual, write that person’s usual monthly income.
c)If anyone is
d)Sign the form and include your Social Security Number in #5. If you do not have a Social Security Number, check the box “Check here if no Social Security Number.”
5.SIGNATURE AND SOCIAL SECURITY NUMBER:
a)The form must have a signature of an adult household member.
b)The adult household member who signs the statement must include his/her Social Security Number. If he/she does not have a Social Security number, check the box “Check here if no Social Security Number”. A Social Security Number is not needed if you listed a Food Stamp, CalWORKs,
6.RACIAL/ETHNIC IDENTITY: You are not required to answer this question to get meal benefits, but completion of this information will help ensure that everyone is treated fairly.
Earnings from Work: Wages/salaries/tips Strike benefits
Unemployment compensation Worker’s compensation
Net income from
Welfare/Child Support/Alimony Public assistance payments Welfare payments Alimony/child support payments
INCOME TO REPORT
Pensions/Retirement/Social Security
Pensions
Supplemental security income Retirement income
Veteran’s payments
Social Security
Other Monthly
Disability benefits
Cash withdrawn from savings Interest dividends
Income from estates/trusts/investments Regular contributions from persons not living in the household
Net royalties/annuities/net rental income Military allowance for
CALIFORNIA DEPARTMENT OF EDUCATION |
CHILD AND ADULT CARE FOOD PROGRAM |
NUTRITION SERVICES DIVISION |
NSD 3101 PAGE 4 (REV. 03/07) |
DESCRIPTION OF RACIAL AND ETHNIC CATEGORIES
The federal government has established the following five racial categories and one ethnic category:
RACIAL:
American Indian or Alaska Native
Asian
Black or African American
Native Hawaiian or Other Pacific Islander - A person having origins in any of the original peoples of Hawaii, Guam, Samoa, or other Pacific Islands.
White
ETHNIC:
Hispanic or Latino