RULES AND PROCEDURE OF THE WORKERS' COMPENSATION BOARD
12NYCRR 300.17 Notices of Retainer, Appearance and Substitution,
and Fees of Claimant's Attorney or Licensed Representative
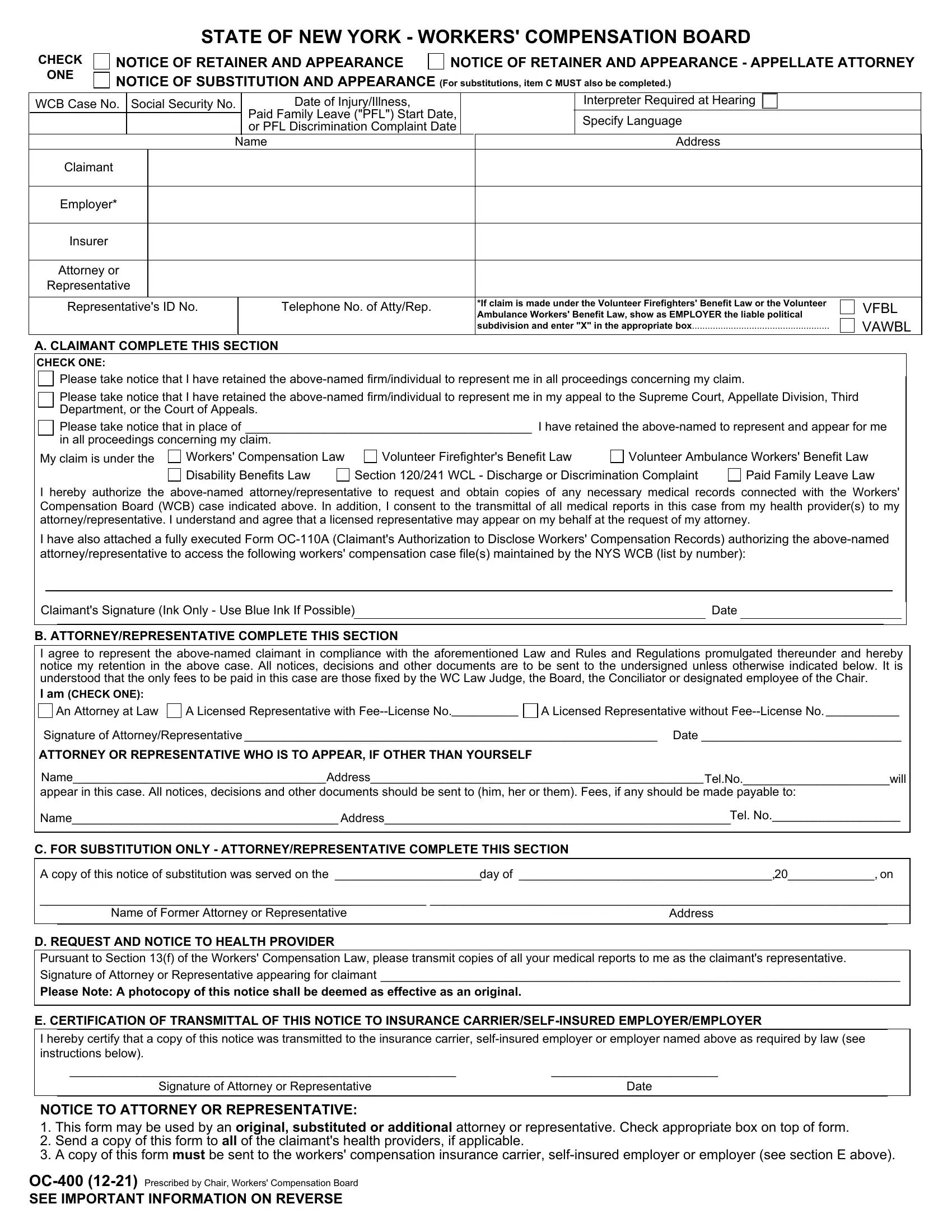
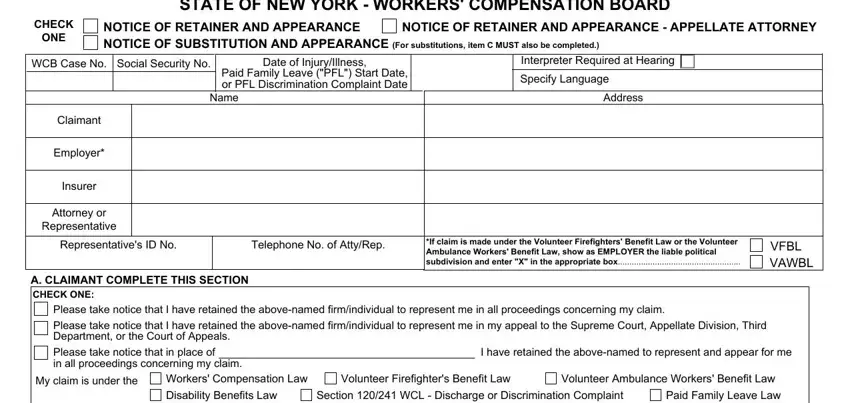
§300.17 Notices of retainer, appearance, substitution and withdrawal, and fees of claimant's attorney or licensed representative. In the representation of a claimant before the board or a Workers' Compensation Law Judge in any case:
a.An attorney or licensed representative shall file a notice of retainer and appearance, and, when appropriate, a notice of substitution, in the format prescribed by the chair, immediately upon being retained. The attorney or licensed representative shall also transmit a copy of such notice to the insurance carrier, self-insured or other representative of the employer at the time of filing.
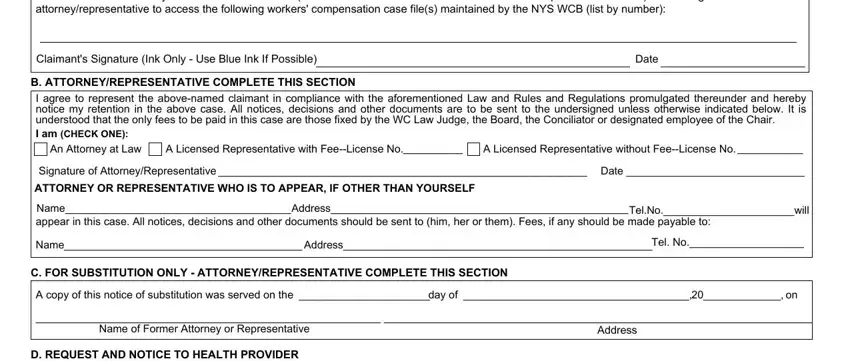
b.1. An attorney or licensed representative, substituted for a former attorney or licensed representative, shall immediately upon being retained serve the former attorney or licensed representative with a copy of the notice of substitution.
2.An attorney or licensed representative may withdraw from representation of a claimant when (i) a notice of substitution has been filed; or (ii) a withdrawal of representation completed in the format prescribed by the Chair has been filed and approved by a Workers’ Compensation Law Judge or conciliator. Failure to obtain the approval of a Workers’ Compensation Law Judge or conciliator prior to ceasing representation of a claimant, when a notice of substitution has not been filed, will constitute the basis of a referral for a violation of Rule 1.16 of the Rules of Professional Conduct (22 NYCRR 1200.0) for an attorney, and may be the basis for license revocation of a licensed representative.
c.No fee shall be approved or fixed, in accordance with subdivision (f) of this section, for the services of any such attorney or licensed representative who has failed or neglected to serve and file the required notice of retainer and appearance, the required notice of substitution, or obtained approval of a withdrawal of representation as required in subparagraph (2) of subdivision (b) herein.
d.1. An attorney or licensed representative shall file an application ]in the format prescribed by the Chair in each instance where a fee is requested pursuant to sections 24 and 24-a of the Workers' Compensation Law, except that where the fee requested is not more than $1000, the attorney or licensed representative may, in lieu of such written application, make an oral statement on the record as to the services rendered and the time spent for the performance of such services. Notwithstanding the foregoing, the board may require an application in the format prescribed by the Chair for a fee of $1000 or less. Any fee application shall be accurately completed.
2.All fees awarded at a hearing are to be made in the presence of the claimant, except that the Workers' Compensation Law Judge may, in his or her discretion, waive this requirement if the amount of the fee requested is not more than $1000, provided that the attorney or licensed representative makes a statement on the record as to the services rendered and the time spent for the performance of such services.
3.In any case where the claimant is not present and the amount of the fee requested is more than $1000, the claimant must be advised of the amount requested by the attorney or licensed representative 10 days in advance of the awarding of a fee. The fee application shall contain a statement signed by the claimant indicating that he or she has reviewed the fee request with the attorney or licensed representative, has no objection to the requested fee, and understands that any approved fee will be deducted from the award, or the attorney or licensed representative shall, together with the fee application, submit written explanation as to why the signature was not obtained. If the board finds insufficient excuse for failure to obtain the written signature, the fee application may be considered defective. Proof of service by mail or otherwise on the copy of the fee application prescribed by the chair and filed with the board, may be accepted as evidence that the claimant has been so advised.
e.Whenever a fee is requested in excess of $1000 for services rendered in conciliation, administrative determination, agreement pursuant to section
32of the Workers' Compensation Law, or conference calendar processing, the request is to be made in the format prescribed by the Chair in each instance where a fee is requested. Such fee request shall be itemized as to the services performed in the time since any prior fee request was submitted and the time spent for each service, with a total amount of time spent. Failure to sufficiently itemize services or time spent on services may be the basis for reducing or denying the fee request. The claimant must be advised of the amount requested, the service rendered and the time spent for the performance of the services by the attorney or licensed representative 10 days prior to the awarding of a fee. Proof of service by mail or otherwise on the copy of the fee request filed with the board, may be acceptable as evidence that the claimant has been so advised. Fees awarded in conciliation, administrative determination, agreement pursuant to section 32 of the Workers' Compensation Law, or conference calendar processing, may be approved by a conciliator or designee of the chair.
f.Whenever an award is made to a claimant who is represented by an attorney or a licensed representative, and a fee is requested, the board in such case shall approve a fee in an amount commensurate with the services rendered and having due regard for the financial status of the claimant and whether the attorney or licensed representative engaged in dilatory tactics or failed to comply in a timely manner with board rules. Unbecoming or unethical conduct by an attorney or licensed representative may result in reduction or denial of a fee request. In no case shall the fee be based solely on the amount of the award.
g.Whenever an attorney or licensed representative is notified, by notice of substitution or otherwise, that the claimant has terminated his or her retainer, the attorney or licensed representative, in each instance where a fee is requested for services rendered for which no previous fee has been approved, shall file an application for such final fee in the format prescribed by the Chair, within thirty days of the filing of the notice of substitution, and serve a copy upon the claimant. The claimant must be advised of the amount requested, the service rendered and the time spent for the performance of the services by the attorney or licensed representative, 10 days prior to the awarding of a fee. Proof of service by mail or otherwise on the copy of a fee request filed with the board, may be acceptable as evidence that the claimant has been so advised. Where the fee requested is not more than $1000, the attorney or licensed representative may make an oral statement on the record as to the services rendered and the time spent for the performance of such services, at the first hearing held following notice to such attorney or licensed representative that the retainer has been terminated.
h.No fee shall be awarded to a claimant's attorney or licensed representative unless the attorney or licensed representative has complied with the requirements of this section.
i.The Chair may require that an attorney or licensed representative with access via the internet to his or her client’s electronic case folder receive Board notices via an electronic mailbox.
It is unlawful to disclose individually identifiable information from Workers' Compensation Board records to any person who is not otherwise lawfully authorized to obtain these records. Any person who knowingly and willfully obtains workers' compensation records which contain individually identifiable information under false pretenses or otherwise violates Workers' Compensation Law Section 110-a shall be guilty of a Class A misdemeanor and shall be subject upon conviction to a fine of not more than one thousand dollars.
NYS Workers' Compensation Board, PO Box 5205, Binghamton, NY 13902-5205
Customer Service: (877) 632-4996