In the state of Michigan, road safety is a paramount concern that is taken seriously by authorities. To ensure the continued safety of all road users, the Department of State has provisions in place for evaluating the driving capabilities of individuals who might pose a risk due to various medical or physical conditions. The OC-88 form, a crucial part of this process, serves as a request for driver evaluation, catering specifically to those instances where physical infirmities, disabilities, vision deficiencies, convulsive seizures, or blackouts could impair a person's ability to drive safely. As dictated by Section 257.320 of the Michigan Vehicle Code, this form initiates a reexamination process that scrutinizes a driver's fitness to be on the road. Encouraging thorough and accurate reporting, the form requires detailed information about the driver in question and an explicit explanation of why an evaluation is deemed necessary. Additionally, it emphasizes the need for complete requester information, including a mandatory signature to process the request, underscoring the form's integrity and confidentiality aspects. The OC-88's structured format and the procedural rigor it represents underscore Michigan's commitment to public safety through responsible driver assessment.
| Question | Answer |
|---|---|
| Form Name | Form Oc 88 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | od 88, michigan form oc 88, oc 88, mi sos oc |
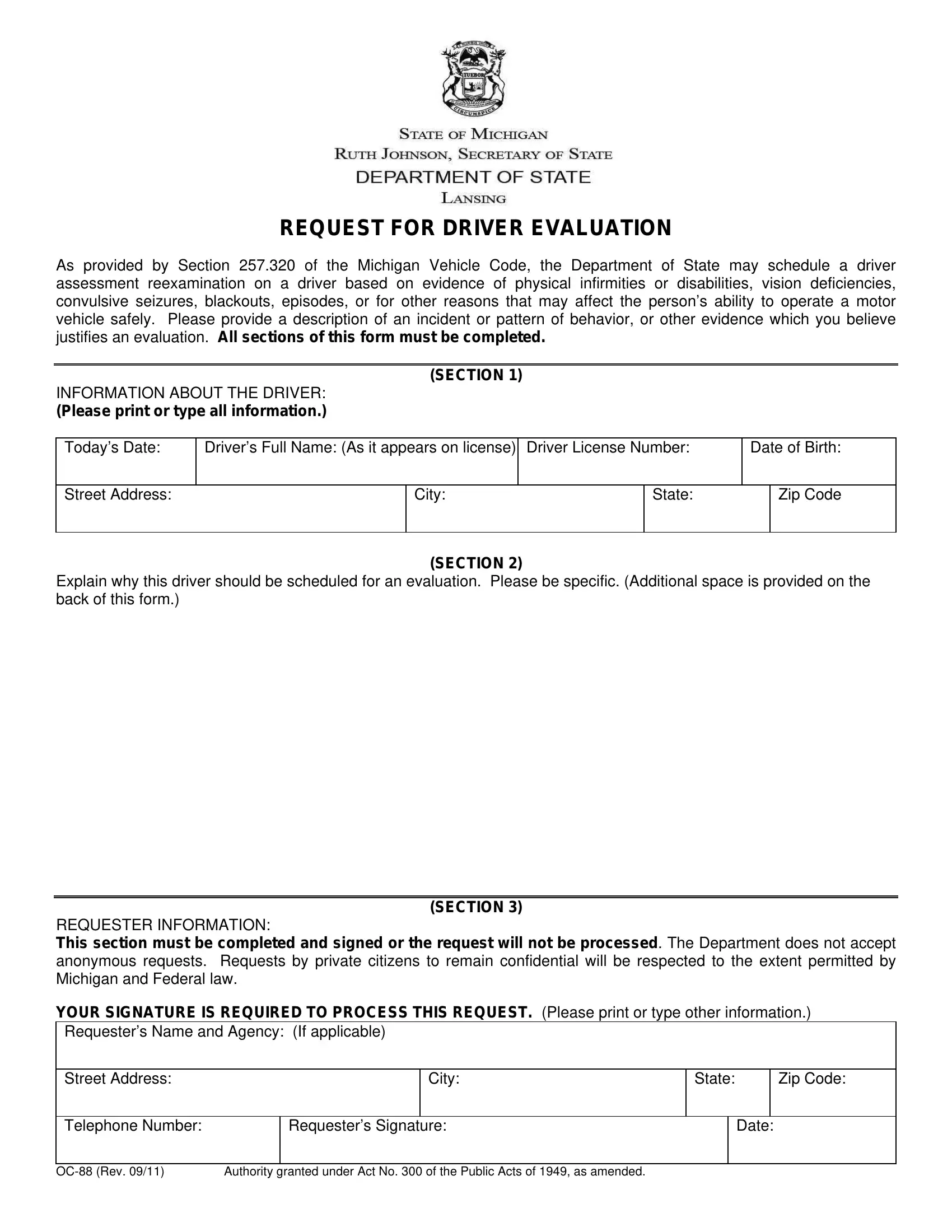
REQUEST FOR DRIVER EVALUATION
As provided by Section 257.320 of the Michigan Vehicle Code, the Department of State may schedule a driver assessment reexamination on a driver based on evidence of physical infirmities or disabilities, vision deficiencies, convulsive seizures, blackouts, episodes, or for other reasons that may affect the person’s ability to operate a motor vehicle safely. Please provide a description of an incident or pattern of behavior, or other evidence which you believe justifies an evaluation. All sections of this form must be completed.
(SECTION 1)
INFORMATION ABOUT THE DRIVER:
(Please print or type all information.)
Today’s Date: |
Driver’s Full Name: (As it appears on license) |
Driver License Number: |
Date of Birth: |
|||
|
|
|
|
|
|
|
Street Address: |
|
City: |
|
State: |
|
Zip Code |
|
|
|
|
|
|
|
(SECTION 2)
Explain why this driver should be scheduled for an evaluation. Please be specific. (Additional space is provided on the back of this form.)
(SECTION 3)
REQUESTER INFORMATION:
This section must be completed and signed or the request will not be processed. The Department does not accept anonymous requests. Requests by private citizens to remain confidential will be respected to the extent permitted by Michigan and Federal law.
YOUR SIGNATURE IS REQUIRED TO PROCESS THIS REQUEST. (Please print or type other information.)
Requester’s Name and Agency: (If applicable)
Street Address:
City:
State:
Zip Code:
Telephone Number:
Requester’s Signature:
Date:
Authority granted under Act No. 300 of the Public Acts of 1949, as amended. |
SECTION 2 (Continued):
Additional Information:
Please attach a copy of any related report(s). The completed form may be mailed or faxed:
Michigan Department of State
Traffic Safety Division
P.O. Box 30810
Lansing, Michigan
Telephone:
Fax: (517)
www.michigan.gov/sos