The child abuse and maltreatment form ocfs nys filling in process is very simple. Our editor allows you to use any PDF form.
Step 1: Choose the orange button "Get Form Here" on this web page.
Step 2: You're now equipped to enhance child abuse and maltreatment form ocfs nys. You have lots of options thanks to our multifunctional toolbar - you'll be able to add, remove, or alter the content, highlight its particular areas, as well as carry out similar commands.
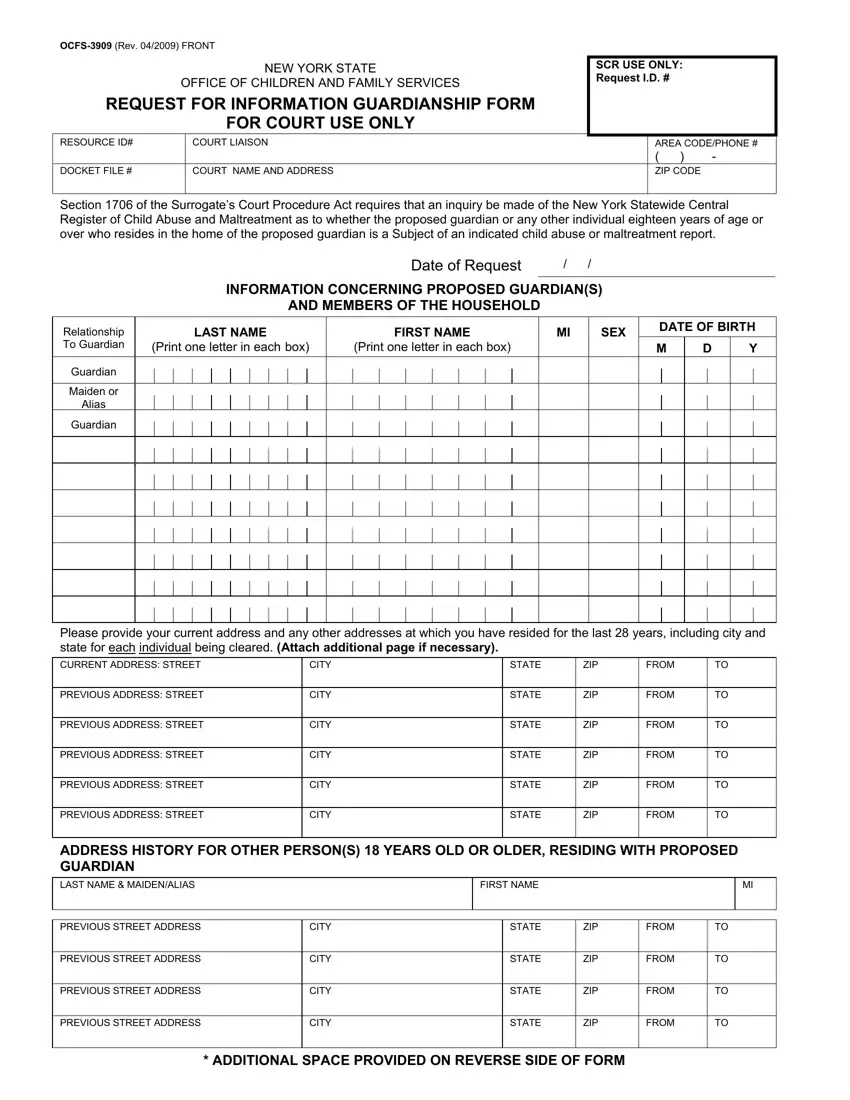
You have to type in the next details to fill out the document:
Put the required details in the PREVIOUS ADDRESS STREET, PREVIOUS ADDRESS STREET, PREVIOUS ADDRESS STREET, PREVIOUS ADDRESS STREET, CITY, CITY, CITY, CITY, STATE, STATE, STATE, STATE, ZIP, ZIP, and ZIP segment.
Put down the necessary data as you are within the LAST NAME, ADDITIONAL ADDRESSES, FIRST NAME, PREVIOUS STREET ADDRESS, CITY, STATE, ZIP, FROM, LAST NAME, FIRST NAME, PREVIOUS STREET ADDRESS, CITY, STATE, ZIP, and FROM segment.
Explain the rights and obligations of the parties inside the box PREVIOUS STREET ADDRESS, CITY, STATE, ZIP, FROM, LAST NAME, FIRST NAME, PREVIOUS STREET ADDRESS, CITY, STATE, ZIP, FROM, TO ORDER A SUPPLY OF OCFS FORMS, and Mail your completed Request for.
Step 3: Hit the Done button to be sure that your completed file can be exported to every electronic device you use or forwarded to an email you indicate.
Step 4: Produce duplicates of your document. This is going to protect you from forthcoming issues. We cannot see or distribute your information, so be certain it will be secure.
