Managing documents using our PDF editor is simpler as compared to anything else. To change ocfs training the form, you'll find nothing for you to do - only adhere to the actions below:
Step 1: The following website page has an orange button that says "Get Form Now". Hit it.
Step 2: Now, you can begin modifying your ocfs training. The multifunctional toolbar is at your disposal - add, delete, alter, highlight, and perform several other commands with the content in the document.
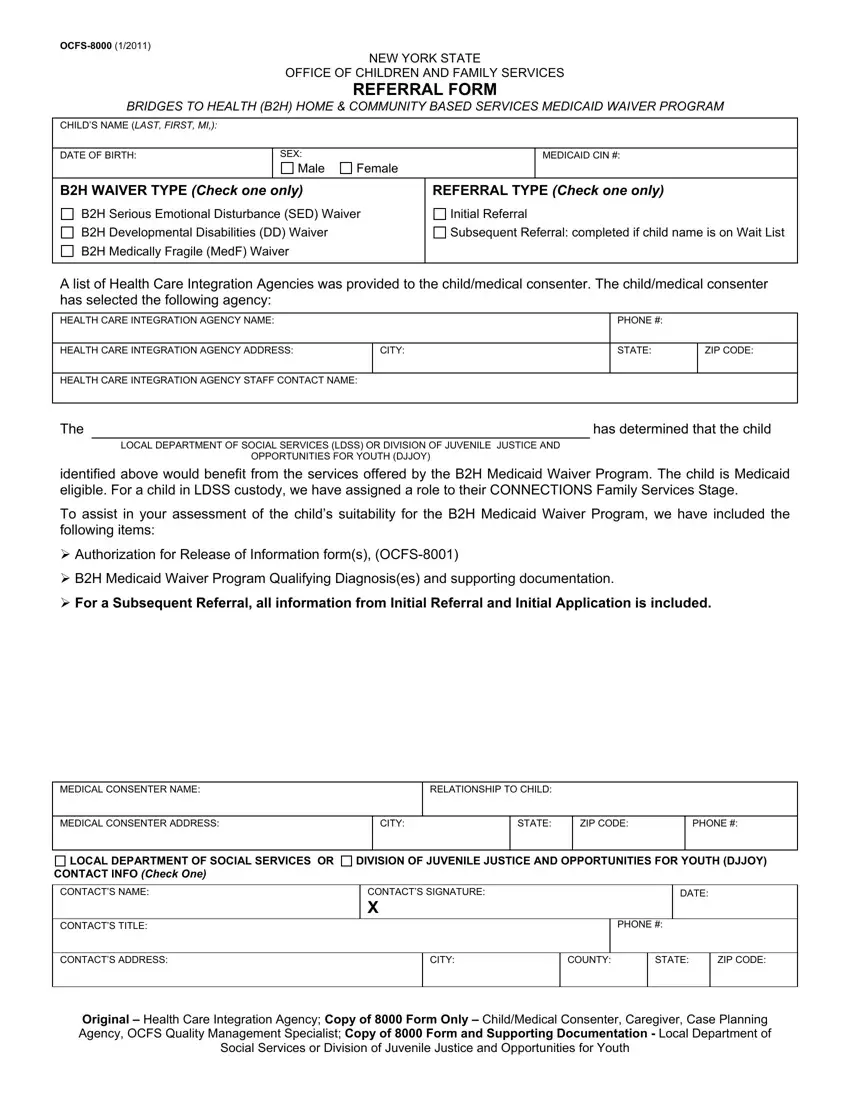
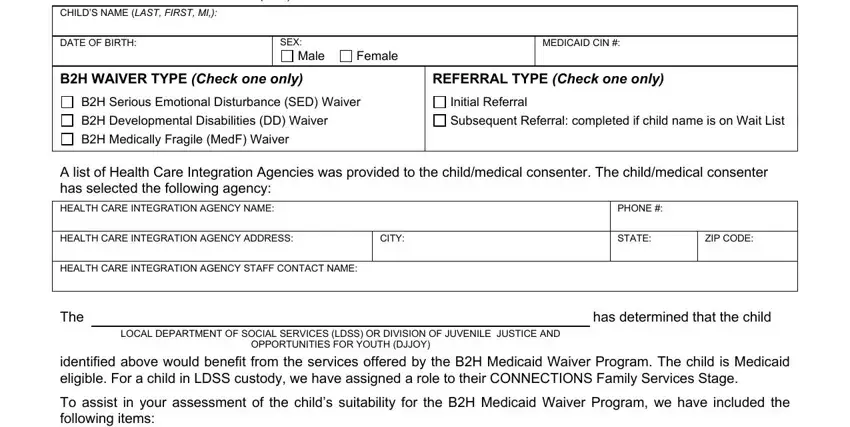
These sections will create the PDF document that you'll be creating:
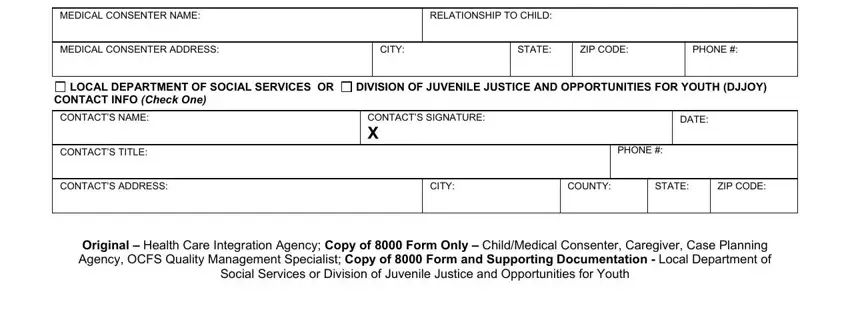
Write down the details in the MEDICAL CONSENTER NAME, RELATIONSHIP TO CHILD, MEDICAL CONSENTER ADDRESS, CITY, STATE, ZIP CODE, PHONE, LOCAL DEPARTMENT OF SOCIAL, DIVISION OF JUVENILE JUSTICE AND, CONTACT INFO Check One, CONTACTS NAME, CONTACTS TITLE, CONTACTS SIGNATURE X, DATE, and PHONE area.
Step 3: Select "Done". You can now transfer the PDF file.
Step 4: Make duplicates of your file - it may help you refrain from potential future complications. And don't get worried - we do not share or check your details.
