
Working with PDF forms online is definitely very easy using our PDF editor. Anyone can fill out dominion power medical form here effortlessly. The tool is consistently maintained by us, getting handy functions and becoming better. To begin your journey, take these simple steps:
Step 1: Open the PDF file in our tool by pressing the "Get Form Button" above on this page.
Step 2: The editor lets you change PDF forms in a range of ways. Improve it by writing personalized text, adjust what's already in the document, and add a signature - all within the reach of a couple of mouse clicks!
As for the blanks of this precise document, here's what you want to do:
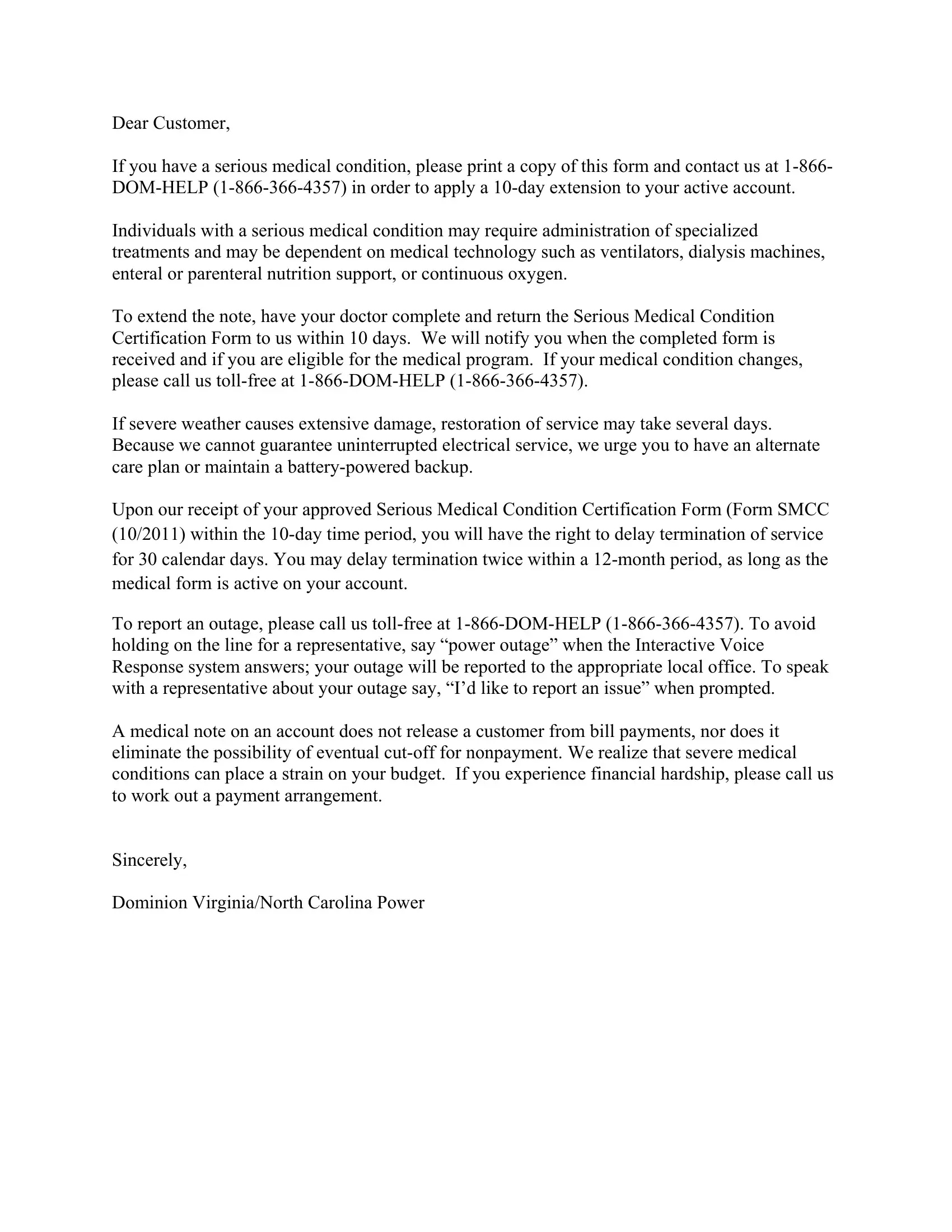
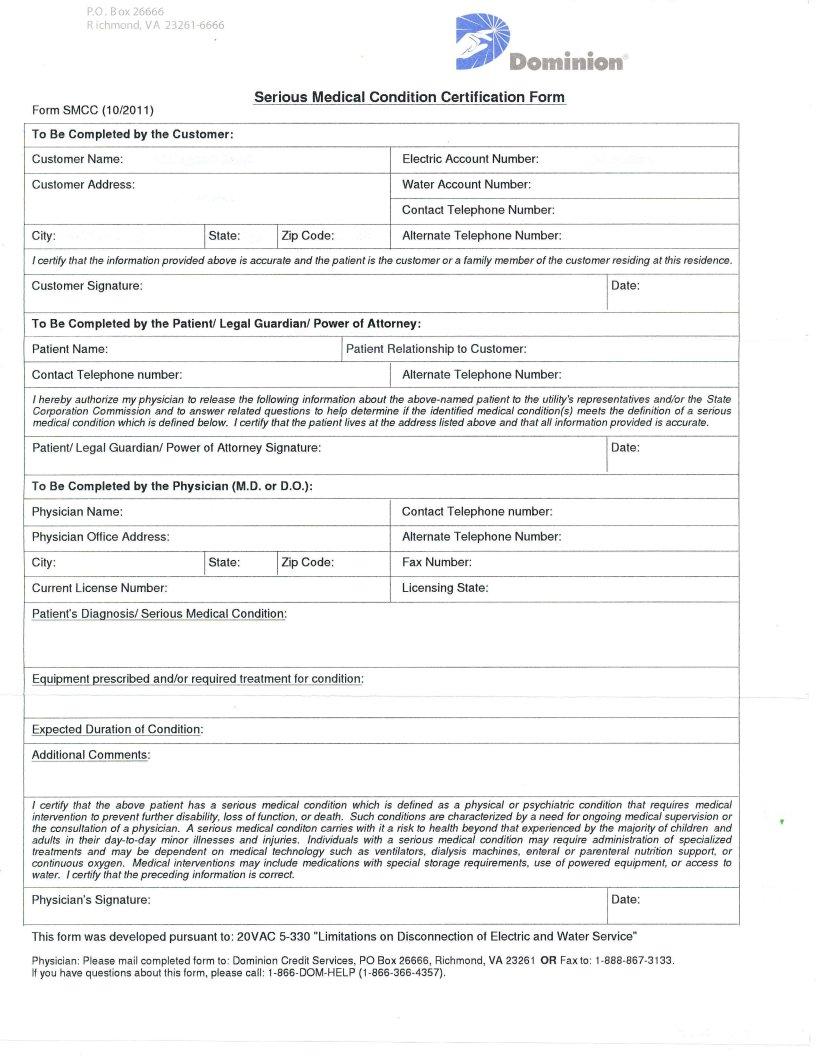
1. Before anything else, once completing the dominion power medical form, beging with the part that features the next blanks:
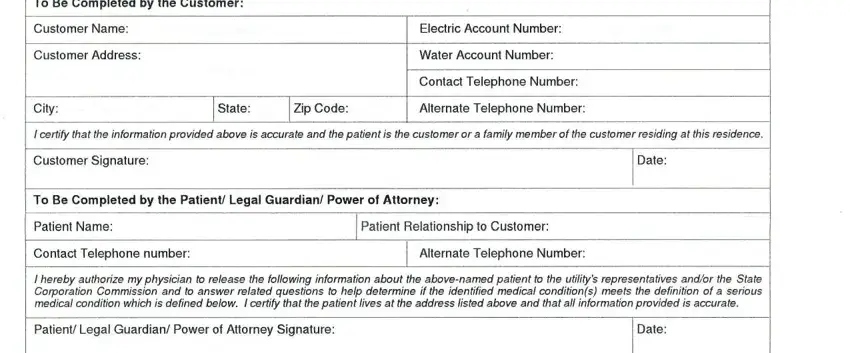
2. Once this array of fields is completed, you're ready add the essential specifics in To Be Completed by the Physician, Physician Name, Physician Olfice Address City, Current License Number, lState lZip Code, Patients Diagnosis Serious Medical, Conlact Telephone number, Alternate Telephone Number, Fax Number, Licensing State, Equipment prescribed andor, Exoected Duration of Condition, Additional Commenls, and I certify that the above patient allowing you to move on further.
People who use this document generally make some mistakes when filling out Exoected Duration of Condition in this section. You should re-examine everything you type in right here.
3. The following segment will be focused on I certify that the above patient, Physicians Signature, Date, This form was developed pursuant, and Physician Pleasemail - type in these blanks.
Step 3: After you have glanced through the information in the fields, press "Done" to conclude your document creation. Make a free trial option with us and acquire immediate access to dominion power medical form - which you may then work with as you want in your personal account. FormsPal is dedicated to the personal privacy of our users; we ensure that all personal data handled by our editor is kept confidential.