Form Omh 270 is one of the most commonly used forms in Ohio. It is used to report wages, tips, and other compensation to the Internal Revenue Service. This form must be filed by employers who have paid employees more than $600 in a calendar year. Knowing how to complete this form correctly is essential for businesses in Ohio. In this blog post, we will walk you through everything you need to know about Form Omh 270. We will explain what each section of the form asks for and provide tips on how to fill it out accurately. Let's get started!
| Question | Answer |
|---|---|
| Form Name | Form Omh 270 |
| Form Length | 7 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min 45 sec |
| Other names | B-2, omh cairs, OMRDD, New_York |
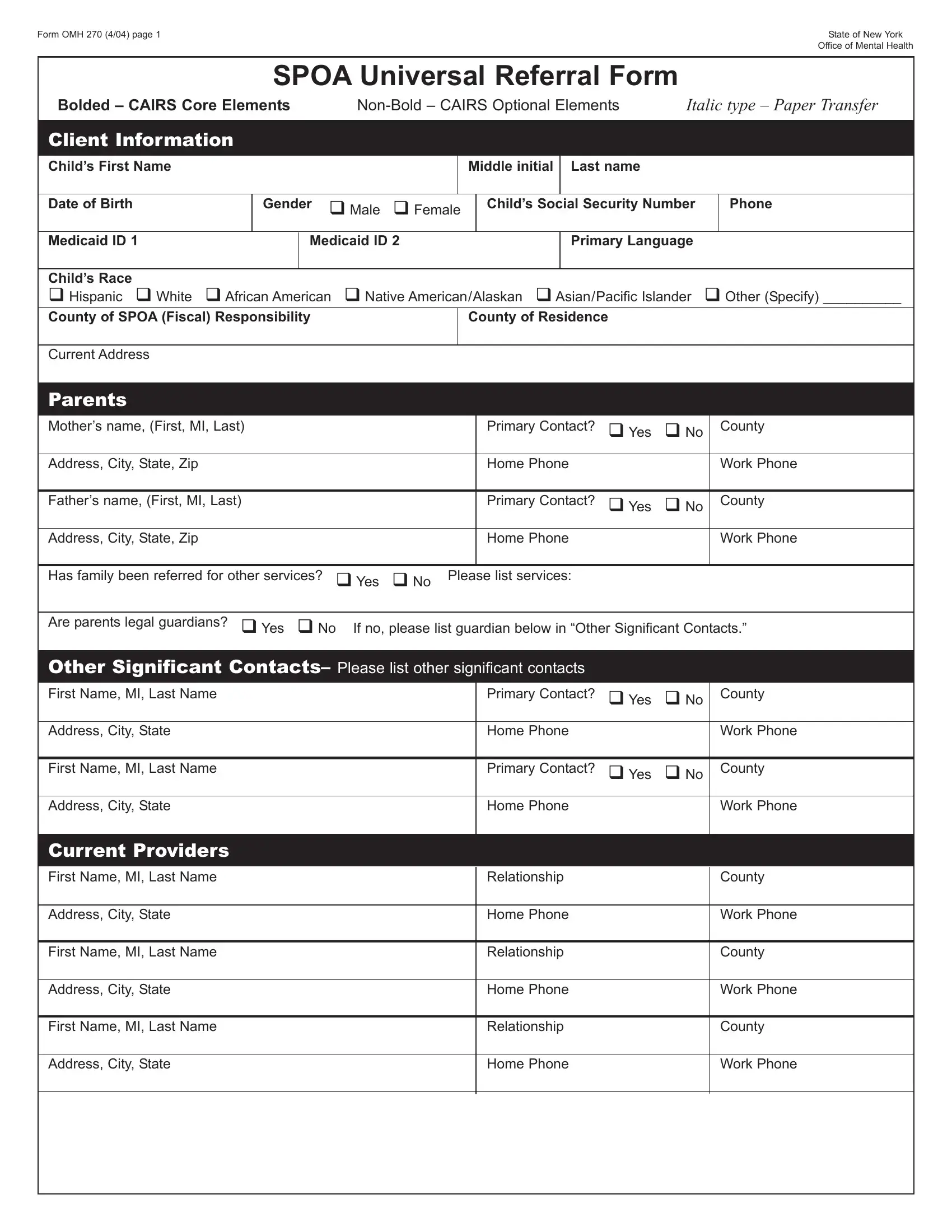
Form OMH 270 (4/04) page 1State of New York Office of Mental Health
SPOA Universal Referral Form
Bolded – CAIRS Core Elements
Client Information |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Child’s First Name |
|
|
|
|
|
|
Middle initial |
Last name |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
||||
Date of Birth |
|
Gender |
ノ Male ノ Female |
Child’s Social Security Number |
|
|
Phone |
|||||||
|
|
|
|
|
|
|
|
|
|
|
||||
Medicaid ID 1 |
|
|
Medicaid ID 2 |
|
|
|
Primary Language |
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Child’s Race |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ノ Hispanic ノ White ノ African American |
ノ Native American/Alaskan ノ Asian/Pacific Islander |
ノ Other (Specify) __________ |
||||||||||||
County of SPOA (Fiscal) Responsibility |
|
|
|
County of Residence |
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Current Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Parents |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Mother’s name, (First, MI, Last) |
|
|
|
|
Primary Contact? |
ノ Yes |
ノ No |
|
|
County |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address, City, State, Zip |
|
|
|
|
|
|
|
Home Phone |
|
|
|
|
Work Phone |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Father’s name, (First, MI, Last) |
|
|
|
|
Primary Contact? |
ノ Yes |
ノ No |
|
|
County |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address, City, State, Zip |
|
|
|
|
|
|
|
Home Phone |
|
|
|
|
Work Phone |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Has family been referred for other services? |
ノ Yes ノ No |
Please list services: |
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|||||
Are parents legal guardians? |
ノ Yes ノ No |
If no, please list guardian below in “Other Significant Contacts.” |
||||||||||||
|
|
|
|
|
|
|
|
|||||||
Other Significant Contacts– Please list other significant contacts |
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
First Name, MI, Last Name |
|
|
|
|
|
|
|
Primary Contact? |
ノ Yes |
ノ No |
|
|
County |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address, City, State |
|
|
|
|
|
|
|
Home Phone |
|
|
|
|
Work Phone |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
First Name, MI, Last Name |
|
|
|
|
|
|
|
Primary Contact? |
ノ Yes |
ノ No |
|
|
County |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address, City, State |
|
|
|
|
|
|
|
Home Phone |
|
|
|
|
Work Phone |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Current Providers |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
First Name, MI, Last Name |
|
|
|
|
|
|
|
Relationship |
|
|
|
|
County |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address, City, State |
|
|
|
|
|
|
|
Home Phone |
|
|
|
|
Work Phone |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
First Name, MI, Last Name |
|
|
|
|
|
|
|
Relationship |
|
|
|
|
County |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address, City, State |
|
|
|
|
|
|
|
Home Phone |
|
|
|
|
Work Phone |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
First Name, MI, Last Name |
|
|
|
|
|
|
|
Relationship |
|
|
|
|
County |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address, City, State |
|
|
|
|
|
|
|
Home Phone |
|
|
|
|
Work Phone |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Form OMH 270 (4/04) page 2 |
State of New York |
|
Office of Mental Health |
SPOA Universal Referral Form
Background Information
Child’s living situation: (Check one box only)
01 |
ノ Independent living |
11 |
ノ DFY Community Group Home |
21 |
ノ Jail |
02 |
ノ Two parent family |
12 |
ノ Family Based Treatment |
22 |
ノ Homeless/streets |
03 |
ノ One parent family |
13 |
ノ OCFS Therapeutic Foster Care |
24 |
ノ Grandparent(s) |
04 |
ノ Two parent adoptive family |
14 |
ノ Crisis Residence |
25 |
ノ Private psychiatric inpatient- Article 31 |
05 |
ノ One parent adoptive family |
15 |
ノ Runaway shelter |
26 |
ノ General hospital psych inpatient- Article 28 |
06 |
ノ Other relative’s home |
16 |
ノ Residential school (SED) |
27 |
ノ State psychiatric inpatient |
07 |
ノ OCFS Family Foster Care |
17 |
ノ Residential Treatment Center (OCFS) |
88 |
ノ Other specify |
08 |
ノ OMH CY Community Residence 18 |
ノ Residential Treatment Facility (OMH) |
99 |
ノ Unknown |
|
09 |
ノ Teaching Family Home |
19 |
ノ Psychiatric inpatient care - unspecified |
|
|
10 |
ノ OCFS Group home |
20 |
ノ OCFS/DRS Facility |
|
|
Child’s custody status: (Check one box only)
01 |
ノ Biological Parents |
04 |
ノ Other Family/Legal Guardians |
06 |
ノ Emancipated Minor |
02 |
ノ Adoptive Parent |
05 |
ノ Local DSS |
88 |
ノ Other |
03 |
ノ Grandparent(s) |
|
|
|
|
Highest level of education completed: (Check one box only)
01 |
ノ Kindergarten |
08 |
ノ Seventh |
15 |
ノ Ungraded – Middle School |
02 |
ノ First |
09 |
ノ Eighth |
16 |
ノ Ungraded – High School |
03 |
ノ Second |
10 |
ノ Ninth |
17 |
ノ College |
04 |
ノ Third |
11 |
ノ Tenth |
18 |
ノ Graduate |
05 |
ノ Fourth |
12 |
ノ Eleventh |
19 |
ノ Post Graduate |
06 |
ノ Fifth |
14 |
ノ Ungraded – Elementary |
99 |
ノ Unknown |
07 |
ノ Sixth |
|
|
|
|
|
|
|
|
|
|
School District: |
|
|
|
|
|
|
|
|
|||
Child’s Educational Placement: (Check one box only) |
|
|
|||
01 |
ノ Regular class in |
10 |
ノ Day Treatment |
||
02 |
ノ Regular class, above grade level |
|
|
11 |
ノ Home instruction |
03 |
ノ Regular class, but behind at least one grade |
12 |
ノ BOCES |
||
04 |
ノ Special class for students with handicapping conditions |
13 |
ノ College |
||
05 |
ノ Residential school for the educationally (emotionally) handicapped |
77 |
ノ Not enrolled in school |
||
06 |
ノ Vocational training only |
|
|
88 |
ノ Other specify |
07 |
ノ Part time vocational/educational |
|
|
99 |
ノ Unknown |
09 |
ノ High school graduate/GED |
|
|
|
|
Home School Name:
Current School Name:
Date of Last IEP:
Committee on Special Education Status:
02 |
ノ Emotionally disturbed |
05 |
ノ Physically disabled |
|
77 |
ノ None |
||||
03 |
ノ Learning disabled |
06 |
ノ Other health impaired |
|
99 |
ノ Unknown |
||||
04 |
ノ Sensory impaired |
07 |
ノ Multiply handicapped |
|
|
|
|
|||
|
|
|
|
|
|
|
||||
Child’s IQ: |
|
Verbal Score– Performance Score: |
|
Full Scale Score: |
|
Date: |
||||
|
|
|
|
|
|
|
||||
Child’s Legal Status: (Check one box only) |
|
|
|
|
||||||
01 |
ノ PINS |
|
04 |
ノ Juvenile delinquent – restricted |
88 |
ノ Other specify |
||||
02 |
ノ PINS Diversion |
|
05 |
ノ Juvenile offender |
|
99 |
ノ Unknown |
|||
03 |
ノ Juvenile delinquent |
77 |
ノ None |
|
|
|
|
|||
Income or benefits child is currently receiving: (Check all that apply)
01 |
ノ Supplemental Security Income (SSI) |
08 |
ノ Medication grant |
02 |
ノ Social Security Disability Income (SSDI) |
09 |
ノ Private insurance, employer coverage, no third party insurance |
03 |
ノ Veteran benefit |
10 |
ノ Other (please specify) ________________________________ |
04 |
ノ Social Security retirement, survivor’s or dependent’s (SSA) |
|
|
05 |
ノ Any public assistance cash program: Family Assistance (TANF), Safety Net, Temporary Disability |
||
06 |
ノ Medicaid |
|
|
07 |
ノ Medicare |
|
|
Form OMH 270 (4/04) page 3 |
|
State of New York |
|
|
Office of Mental Health |
SPOA Universal Referral Form |
|
|
|
|
|
Other Benefits (Annual or Monthly Amounts) |
|
|
|
|
|
Insurance Type, Policy Holder, Policy Number: |
Citizenship: ノ Yes ノ No |
Legal Alien: ノ Yes ノ No |
Income: |
|
Date of Entry: ___________________ |
|
|
|
HI number, currently enrolled? ノ Yes ノ No |
|
Country of Origin: ________________ |
Child Support (Specific Amounts): ノ Yes ノ No |
|
Alien ID number: _________________ |
Resources/Assets (savings bonds, trust) type & amount: |
|
|
|
|
|
TANE Eligibility (low income, public assistance): |
|
|
Diagnosis Information
Axis I Diagnoses: clinical disorders, other conditions that may be a focus of clinical attention – Up to 4 diagnoses may be entered. Please list Axis 1 Primary Diagnosis first.
Axis II Diagnosis: personality disorders, mental retardation (if any) – Up to 4 diagnoses may be entered
Axis III Diagnosis: general medical conditions (if any) – Up to 4 diagnoses may be entered
Axis IV Diagnosis: psychosocial and environmental problems
1 |
ノ Problems with primary support group |
6 |
ノ Economic problems |
2 |
ノ Problems related to the social environment |
7 |
ノ Problems with access to health care services |
3 |
ノ Educational problems |
8 |
ノ Problems related to access with the legal system/crime |
4 |
ノ Occupational problems |
9 |
ノ Other psychosocial and environmental problems |
5 |
ノ Housing problems |
|
|
Axis V: Global Assessment of Functioning (GAF):
Who Made the Diagnosis:
Symptoms and Behavior
Date of Diagnosis:
Using the scale below, indicate the degree of the child’s symptoms/behaviors.
SCALE
0NOT EVIDENT Child does not display this symptom/ behavior
1MILD This symptom/behavior exists, but there is no impairment (loss of effectiveness) in carrying out daily activities or in meeting major role requirements.
2MODERATE This symptom/behavior exists. This child maintains an appropriate level of functioning in daily activities and major roles only with difficulty and increased effort and support.
3MARGINALLY SEVERE This symptom/behavior exists. There is definite impairment in carrying out daily activities and/or performing major roles. Major roles are able to be perform
4SEVERE This
9 UNKNOWN
DURATION SCALE
1= in past 30 days 2= with in 90 days
3= with in past 6 months 4= with in past year 5= over 1 year
|
|
|
|
|
Margin- |
|
|
|
|
Not |
|
Mod- |
ally |
|
|
|
|
Evident |
Mild |
erate |
Severe |
Severe |
Unknown |
|
|
0 |
1 |
2 |
3 |
4 |
9 |
35 |
Suicidal Ideation |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
36 |
Psychotic Symptoms |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
37 |
Depression |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
38 |
Anxiety |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
39 |
Phobia |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
40 |
Danger to self |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
41 |
Danger to others |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
42 |
Temper Tantrums |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
43 |
Sleep Disorders |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
44 |
Enuresis/Encopresis |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
45 |
Physical Complaints |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
46 |
Alcohol abuse |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
47 |
Drug abuse |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
48 |
Developmental Delays |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
49 |
Sexually inappropriate |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
50 |
Sexually Aggressive |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
51 |
Verbally Aggressive |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
52 |
Physically Aggressive |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
53 |
Eating Disorder |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
54 |
Peer Interactions |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
55 |
Hyperactive |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
56 |
Impulsive |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
57 |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
|
58 |
Runaway |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
Form OMH 270 (4/04) page 4 |
State of New York |
|
Office of Mental Health |
SPOA Universal Referral Form
Using the scale below, indicate the level that most accurately reflects the frequency with the child engaged in the following behaviors in the past 18 months.
SCALE
0 NEVER This behavior not observed or reported.
1RARELY The child has engaged in behavior once in the past 18 months.
2SOMETIMES The child has engaged in behavior two times in the past 18 months.
3OFTEN The child has engaged in behavior five times in the past 18 months.
4ALWAYS The child has routinely engaged in behavior more than five times in the past 18 months.
9 UNKNOWN
|
|
|
|
Some- |
|
|
|
|
|
Never |
Rarely |
times |
Often |
Always |
Unknown |
|
|
0 |
1 |
2 |
3 |
4 |
9 |
44 |
Suicide Attempts |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
45 |
Destruction of Property |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
46 |
Fire Setting |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
47 |
Cruelty to Animals |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
Functioning
SCALE
0 NOT EVIDENT Child does not display this symptom/behavior
1 MILD This symptom/behavior exists, but there is no impairment (lost of effectiveness) in carrying out daily activities or in meeting major role requirements.
2MODERATE This symptom/behavior exists. This child maintains an appropriate level of functioning in daily activities and major roles only with difficulty and increased effort and support.
3 MARGINALLY SEVERE This symptom/behavior exists There is definite impairment in carrying out daily activities and/or performing major roles. Major roles are able to be perform.
4SEVERE This symptom/behavior exists Definite impairment exists in daily activities. The child is unable to perform one or more major role at any level. The child may not be allowed to remain in one or more major roles due to severity of symptom/behavior
9 UNKNOWN
|
|
|
Margin- |
|
|
Not |
|
Mod- |
ally |
|
|
Evident |
Mild |
erate |
Severe |
Severe |
Unknown |
0 |
1 |
2 |
3 |
4 |
9 |
55Self Care
56Social Relationships/Functioning
57Cognitive Functioning/Communication
58Self Direction
59Motor Functioning
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
ノ |
Physical Health Information
Current Medical Conditions:
Any Medical Alerts:
Drugs for Medical Conditions:
Is Child taking medications for psych condition? ノ ノ Yes No
Child’s Treatment and Services History
Medication Name: (if yes is checked)
SCALE
0 Never
1 Not at all in past six months
2One or more times in the past 6 months, but not in the past 3 months
3One or more times in the past 3 months, but not in the past month
4One or more times in the past month, but not in the past week
5 One or more times in the past week
|
(Enter number. Please enter 0 for none.) |
Psychiatric hospitalization in last 12 months |
___________________ |
Psychiatric hospitalization in last 6 months |
___________________ |
Emergency Room visits in last 12 months- NYC only |
___________________ |
Emergency Room visits in last 6 months |
___________________ |
Arrests in last 6 months |
___________________ |
Incarceration in last 6 months |
___________________ |
How frequently was this recipient a victim of sexual or physical abuse?
History of Past and Present Services: (Check all that apply)
01 |
ノ Intensive Case Management |
11 |
ノ Vocational training |
22 |
ノ Flexible funding |
02 |
ノ Service coordination/case management |
12 |
ノ ADL or Independent living skills |
23 |
ノ Foster Care |
03 |
ノ Individualized care coordination |
13 |
ノ Alcohol abuse treatment |
24 |
ノ State psychiatric facility |
04 |
ノ Clinic treatment |
14 |
ノ Substance abuse treatment |
25 |
ノ Private psychiatric facility |
05 |
ノ Private/individual therapy |
15 |
ノ Family Support Services |
26 |
ノ General hospital psychiatric inpatient |
06 |
ノ Crisis response services |
16 |
ノ Transportation |
27 |
ノ OMRDD Developmental Center |
07 |
ノ Home Based Crisis Intervention |
17 |
ノ After school/weekend program |
28 |
ノ Intensive in home |
08 |
ノ Day Treatment |
18 |
ノ Specialized summer program |
29 |
ノ CCSI |
09 |
ノ Respite |
19 |
ノ Specialized educational services |
30 |
ノ Supportive Case Manager |
10 |
ノ Medication management |
20 |
ノ Speech & language therapy |
31 |
ノ Residential Treatment Facility |
|
|
21 |
ノ Mentoring |
88 |
ノ Other specify |
Form OMH 270 (4/04) page 5 |
|
|
|
State of New York |
|
|
|
|
|
|
Office of Mental Health |
|
|
SPOA Universal Referral Form |
|
|
|
|
|
|
|
|
|
Referral |
|
|
|
|
|
|
|
|
|
|
|
Referral Source to SPOA: |
|
|
|
|
|
01 |
ノ Family/legal guardian |
07 |
ノ Social Services |
13 |
ノ Residential Treatment Facility |
02 |
ノ Self |
08 |
ノ Other mental health program |
14 |
ノ Community residence |
03 |
ノ School/education system |
09 |
ノ Physician |
15 |
ノ Intensive Case Management |
04 |
ノ |
11 |
ノ Emergency room |
16 |
ノ OMRDD |
05 |
ノ Local hospital acute inpatient unit |
|
(psychiatric & general hospital) |
88 |
ノ Other specify |
06 |
ノ Juvenile justice system |
12 |
ノ Private psychiatric inpatient hospital |
|
|
Services Child referred to SPOA for: (Check all that apply)
01 |
ノ Intensive Case Management |
11 |
ノ Vocational training |
22 |
ノ Flexible funding |
02 |
ノ Service coordination/case management 12 |
ノ ADL or Independent living skills |
23 |
ノ Foster Care |
|
03 |
ノ Individualized care coordination |
13 |
ノ Alcohol abuse treatment |
24 |
ノ State psychiatric facility |
04 |
ノ Clinic treatment |
14 |
ノ Substance abuse treatment |
25 |
ノ Private psychiatric facility |
05 |
ノ Private/individual therapy |
15 |
ノ Family Support Services |
26 |
ノ General hospital psychiatric inpatient |
06 |
ノ Crisis response services |
16 |
ノ Transportation |
27 |
ノ OMRDD Developmental Center |
07 |
ノ Home Based Crisis Intervention |
17 |
ノ After school/weekend program |
28 |
ノ Intensive in home |
08 |
ノ Day Treatment |
18 |
ノ Specialized summer program |
29 |
ノ CCSI |
09 |
ノ Respite |
19 |
ノ Specialized educational services |
30 |
ノ Supportive Case Manager |
10 |
ノ Medication management |
20 |
ノ Speech & language therapy |
31 |
ノ Residential Treatment Facility |
|
|
21 |
ノ Mentoring |
88 |
ノ Other specify |
Please describe why child requires the highest level of service that SPOA provides:
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
List Child’s Strengths: (Enter as many as desired)
_____________________________________________________________________________________________________
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
List of Family/Caregiver Strengths: (Enter as many as desired)
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
Name of Person Referring Child to SPOA:
Title:
Signature of Person Referring Child to SPOA:
Phone:
Date of Referral to SPOA
Form OMH 270 (4/04) page 6 |
State of New York |
|
Office of Mental Health |
SPOA Universal Referral Form
AUTHORIZATION FOR RELEASE OF INFORMATION
This authorization must be completed by the patient or his/her personal representative to use/disclose protected health information, in accor- dance with State and Federal laws and regulations. A separate authorization is required to use or disclose confidential related information.
PART 1: Authorization for Release of Information
Description of Information to be Used/Disclosed:
I, ____________________________________________________________________, consent to release clinical information to the
Single Point of Access (SPOA). I understand that the SPOA will review and evaluate the information to determine eligibility for services in Home and Community Based Services Waiver, Case Managements Services, Family Based Treatment or Community Residence.
Purpose or Need for Information:
1.This information is being requested by:
ノThe individual or his/her personal representative; or
ノOther (please describe) _______________________________________________________________________________
2.The purpose of the disclosure is (please describe):
It is understood that this information will be used to evaluate ________________________________________ for possible place-
ment with HCBS Wavier, Case Management, Family Based Treatment or Community Residence. Upon acceptance, my child will be receiving services from one of the above.
To: Name, Address, & Title of Person/Organization/Facility Program to Which this Disclosure is to be Made
Note: If the same information is to be disclosed to multiple parties for the same purpose, for the same period of time, this authorization will apply to all parties listed here.
A.I authorize the SPOA to release clinical information and make recommendations for the appropriate program for possible enrollment. I also understand that the SPOA may recommend other appropriate programs/services, such as Residential Treatment Facility, the Coordinated Children’s Services Initiative, or the Parent Resource Center. I hereby permit the use or disclosure of the above infor- mation to the Person/Organization/Facility/Program(s) identified above. I understand that:
1.Only this information may be used and/or disclosed as a result of this authorization.
2.This information is confidential and cannot legally be disclosed without my permission.
3.If this information is disclosed to someone who is not required to comply with federal privacy protection regulations, then it may be redisclosed and would no longer be protected.
4.I have the right to revoke (take back) this authorization at any time. My revocation must be in writing on the form provided to me by ______________________________________________________________. I am aware that revocation will not be effective if the persons I have authorized to use and/or disclose my protected health information have already taken action because of my earlier authorization.
5.I do not have to sign this authorization and that my refusal to sign will not affect my ability to obtain treatment from the New York State Office of Mental Health, nor will it affect my eligibility for benefits.
6.I have a right to inspect and copy my own protected health information to be used and/or disclosed in accordance with the require- ments of the federal privacy protection regulations found under 45 CFR (164.524).
Continue on Next Page
Form OMH 270 (4/04) page 7 |
State of New York |
|
Office of Mental Health |
SPOA Universal Referral Form
Please select one choice from either
My authorization will expire:
ノWhen acted upon;
ノ90 Days from this Date;
My authorization will expire:
ノWhen I am no longer receiving services from one of the intensive high end mental health services;
ノOne Year from this Date;
ノOther ___________________________________________________________________________________
C. Patient Signature: I certify that I authorize the use of my medical/mental health information as set forth in this document.
___________________________________________________________________________ ________________________________
Signature of Patient or Personal Representative |
Date |
___________________________________________________________________________ |
|
Patient’s Name (Printed) |
|
___________________________________________________________________________ |
|
Personal Representative’s Name (Printed) |
|
____________________________________________________________________________________________________________________
Description of Personal Representative’s Authority to Act for the Patient (required if Personal Representative signs Authorization)
D.Witness Statement/Signature: I have witnessed the execution of this authorization and state that a copy of the signed authorization was provided to the patient and/or the Personal Representative
WITNESSED BY: __________________________________________________________ |
________________________________ |
Staff person’s name and title |
Date |
Authorization Provided To: ____________________________________________ |
|
|
|
To be Completed by Facility: |
|
___________________________________________________________________________ |
________________________________ |
Signature of Staff Person Using/Disclosing Information |
Date Released |
___________________________________________________________________________ |
|
Title |
|
PART 2: Revocation of Authorization to Release Information
I hereby revoke my authorization to use/disclose information indicated in Part 1, to the Person/Organization/Facility Program whose name and address is:
___________________________________________________________________________________________________________________
___________________________________________________________________________________________________________________
___________________________________________________________________________________________________________________
I hereby revoke my authorization to use/disclose information indicated in Part 1, to the Person/Organization/Facility Program whose name and address is:
___________________________________________________________________________________________________________________
___________________________________________________________________________________________________________________
___________________________________________________________________________________________________________________
___________________________________________________________________________ |
________________________________ |
Signature of Patient or Personal Representative |
Date |
___________________________________________________________________________ |
|
Patient’s Name (Printed) |
|
___________________________________________________________________________ |
|
Personal Representative’s Name (Printed) |
|
____________________________________________________________________________________________________________________
Description of Personal Representative’s Authority to Act for the Patient (required if Personal Representative signs Authorization)