OFFICE OF STATEWIDE HEALTH PLANNING AND DEVELOPMENT
FACILITIES DEVELOPMENT DIVISION
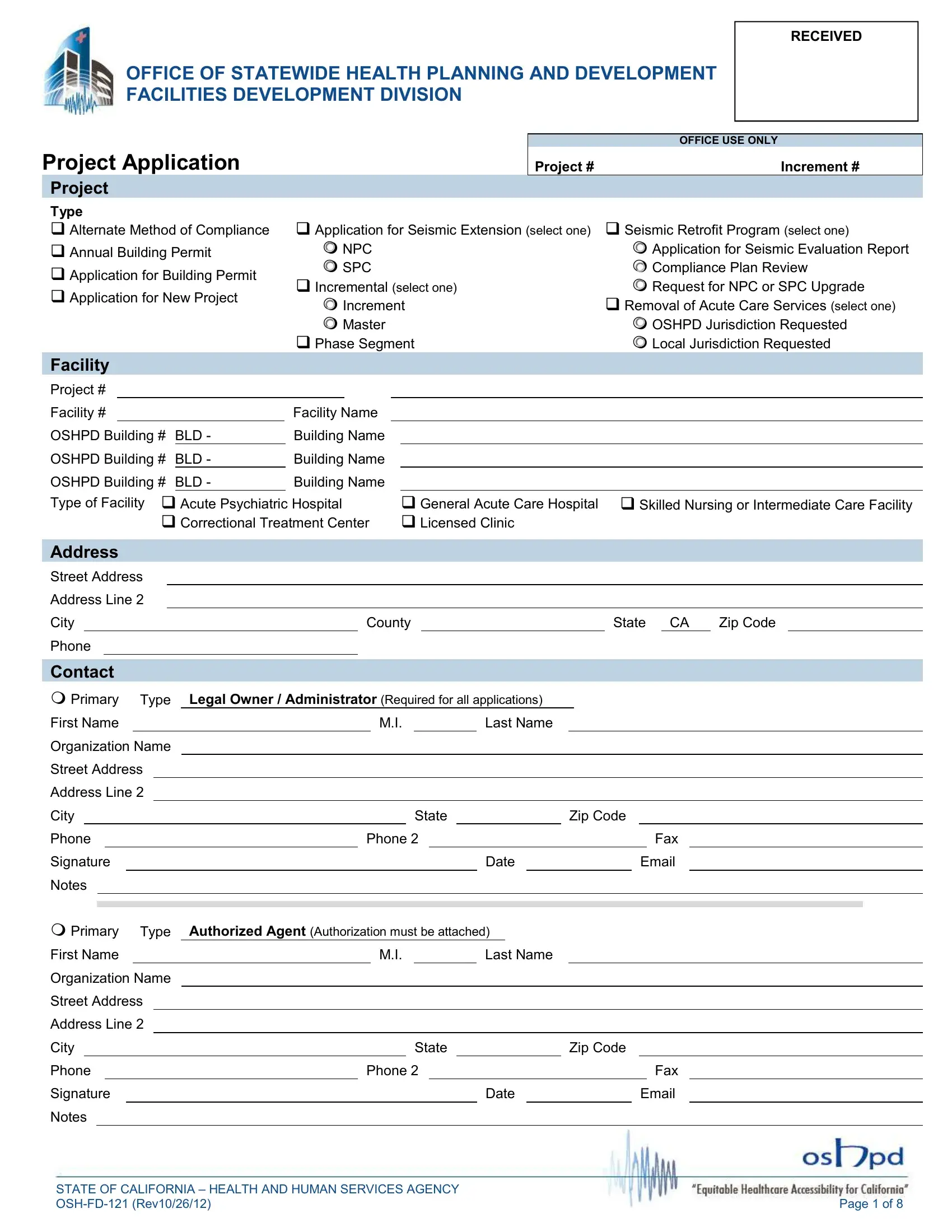
INSTRUCTIONS FOR APPLICATION FOR NEW PROJECT (OSH-FD-121)
This form is required for all application submittals and is to be accompanied by all required project specific forms.
Note: If licensure by the California Department of Public Health is not required by your facility, review by OSHPD is not required; therefore this application is not required. Contact the local jurisdiction for submittal requirements.
Project
The selected box indicates the type of application for submittal.
Facility
•Enter the Office of Statewide Health Planning and Development (OSHPD) facility identification number. If this application is for construction of a new facility and an OSHPD facility identification number has not yet been assigned, contact the office for this number.
•Enter the name of the facility as it appears on the facility license.
•Enter the building number and name which the requested work is to be performed.
•Check the box for the type of facility as it is licensed.
Address
•Enter the facility street address, city, county, zip code and phone number.
Contact
Note: Copies of all correspondence will be sent to the facility representative. If a facility representative address is not entered, copies of all correspondence will be sent to the facility address as indicated on the license, to the attention of Facility Administrator.
•Enter the contact information for the legal owner / administrator (this information is required for all applications) , authorized agent, and facility representative. Include the name, organization name, street address, city, state, zip code, phone number, fax number and email address. Information for accounting, applicant, and billing is optional. If additional space is needed, duplicate this page.
•A signature and date are required for the legal and authorized agent. If an authorized agent is signing on behalf of the legal owner /administrator, the authorization must be attached.
•Indicate who will be the primary contact for this project.
•Provide any additional information in the notes area, as necessary.
Record Detail
•Enter the record/project name.
•Enter a detailed description of the work to be performed.
Application Specific Information – Plan Review
•Indicate the type of submittal for this project by placing a check in the appropriate box. If selecting a collaborative review, phased review or collaborative phased review, complete the Phase Master Plan section.
•Indicate if a managed project review is requested. Refer to Title 24, California Administrative Code, Section 7-111, Definitions.
•If preliminary or final is checked as the type of submittal, enter the date of the presubmittal meeting (for projects with an estimated construction cost greater of $20 million and above).
•Check the box for the kind of project. Refer to Title 24, California Administrative Code, Section 7-111, Definitions.
•Enter the total bed count before construction and after construction. If the bed count is not being affected by this project, this information is not required.