
If you need to fill out form pharmacy template, you won't have to download any software - simply give a try to our PDF editor. We are aimed at giving you the ideal experience with our editor by constantly releasing new features and upgrades. Our editor is now much more helpful as the result of the most recent updates! So now, filling out PDF documents is simpler and faster than ever before. Here's what you'll need to do to start:
Step 1: Click on the "Get Form" button in the top part of this page to access our editor.
Step 2: Using this state-of-the-art PDF file editor, you could do more than simply fill out blank fields. Edit away and make your forms appear faultless with customized textual content put in, or tweak the file's original input to perfection - all accompanied by the capability to incorporate stunning photos and sign it off.
It is actually an easy task to finish the form following this detailed tutorial! Here's what you should do:
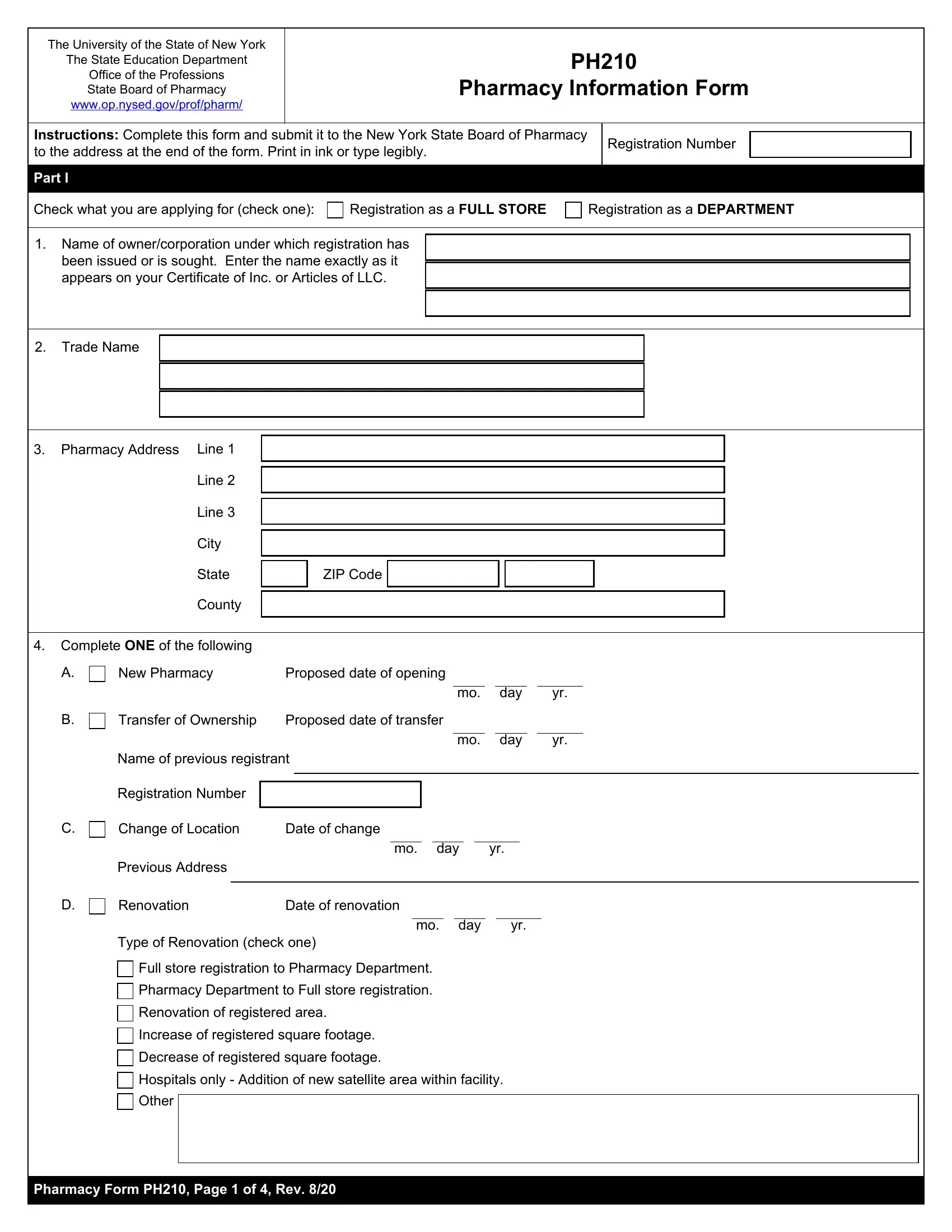
1. Fill out the form pharmacy template with a group of essential fields. Gather all the important information and be sure not a single thing missed!
2. After finishing the previous step, head on to the subsequent part and fill in all required particulars in all these blank fields - State, County, ZIP Code, Complete ONE of the following, New Pharmacy, Proposed date of opening, Transfer of Ownership, Proposed date of transfer, day, day, Name of previous registrant, Registration Number, Change of Location, Date of change, and day.
3. Completing Hospitals only Addition of new, Other, and Pharmacy Form PH Page of Rev is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!

It is possible to make a mistake when completing the Pharmacy Form PH Page of Rev, consequently make sure you look again before you decide to finalize the form.
4. To move forward, this fourth step requires filling in a couple of fields. These include Pharmacy Description Provide a, Do you have, A A sink with hot cold running, B A separate refrigerator for, C Basement storage, D A security system, Daily schedule of hours that, Yes, Yes, Yes, Yes, and Include a photo of front exterior, which you'll find vital to carrying on with this particular PDF.
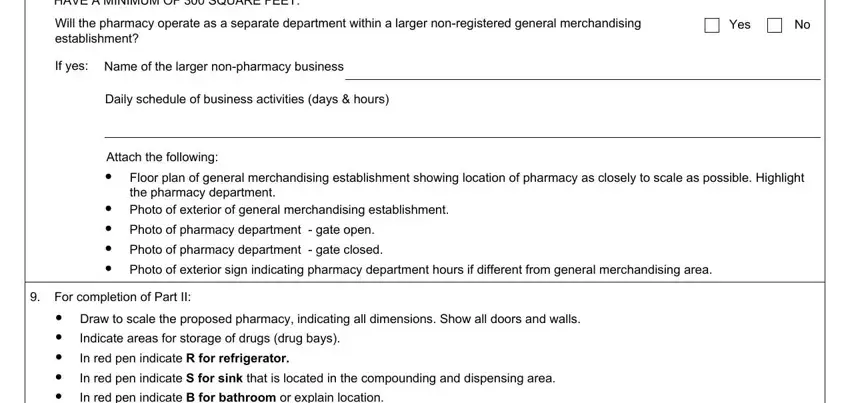
5. To finish your form, this final subsection has a few additional blank fields. Filling out comprising the pharmacy shall be, Will the pharmacy operate as a, Yes, If yes, Name of the larger nonpharmacy, Daily schedule of business, Attach the following, Floor plan of general, Photo of pharmacy department gate, Photo of pharmacy department gate, Photo of exterior sign indicating, For completion of Part II, In red pen indicate B for bathroom, Indicate areas for storage of, and In red pen indicate R for is going to finalize the process and you can be done in an instant!
Step 3: Prior to addressing the next stage, it's a good idea to ensure that blank fields have been filled in the correct way. As soon as you’re satisfied with it, press “Done." Sign up with us today and easily use form pharmacy template, available for downloading. Each edit made is conveniently preserved , enabling you to change the form further if required. FormsPal offers protected document editor with no personal data record-keeping or sharing. Rest assured that your details are in good hands with us!