The purpose of the PME 01 form is to establish the City's contracting process and procedures. Contractors must complete and submit this form in order to be considered for a contract with the City. The form includes information about the contractor's company, qualifications, experience, and contact information. Submission of the PME 01 form is also required for subcontractors working on a City contract. Completing and submitting this form is an essential step in doing business with the City.
| Question | Answer |
|---|---|
| Form Name | Form Pme 01 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | non legend drug permit ct form |
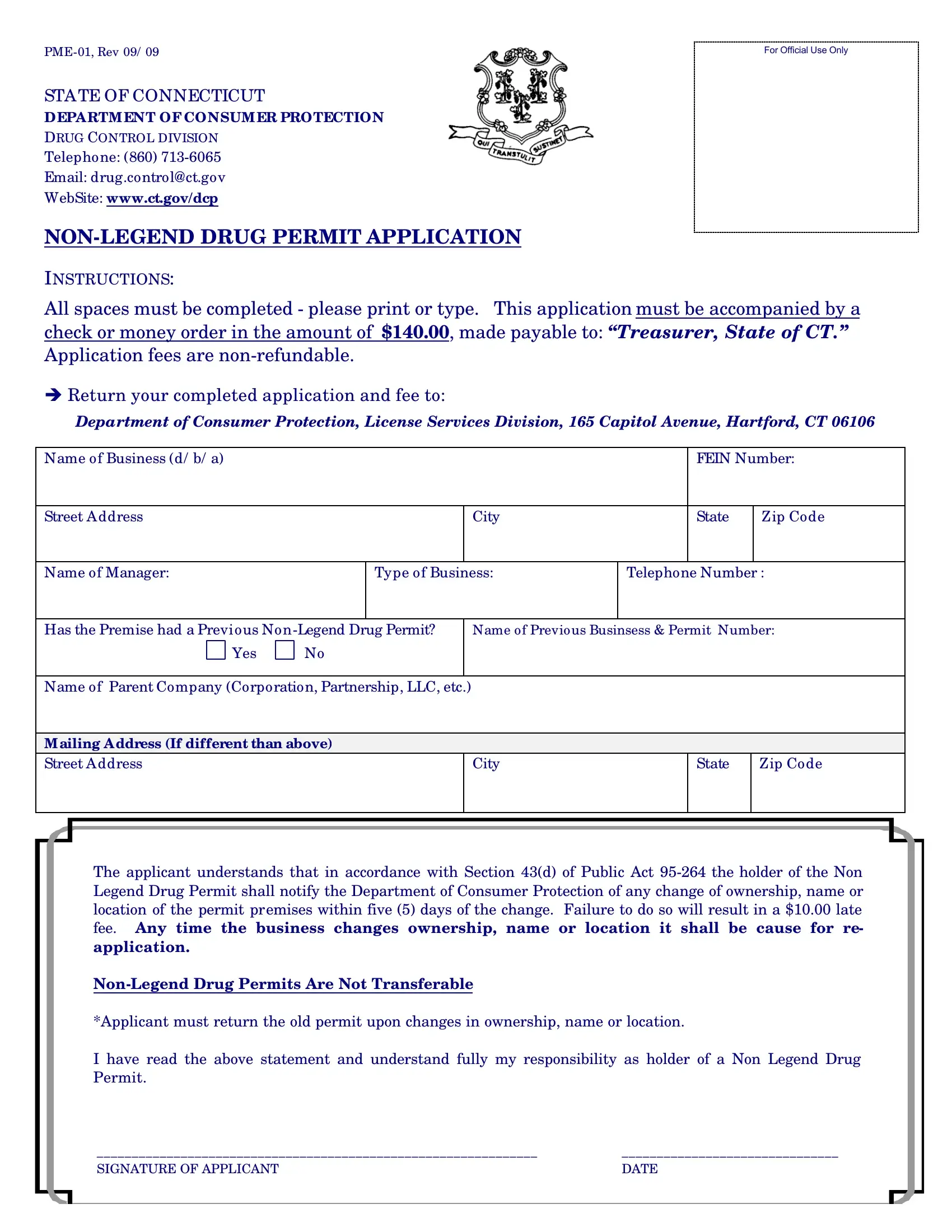
STATE OF CONNECTICUT
DEPA RTM ENT OF CONSUM ER PROTECTION
DRUG CONTROL DIVISION
Telephone: (860)
Email: drug.control@ct.gov
WebSite: www.ct.gov/dcp
INSTRUCTIONS:
For Official Use Only
All spaces must be completed - please print or type. This application must be accompanied by a check or money order in the amount of $140.00, made payable to: “Treasurer, State of CT.” Application fees are
èReturn your completed application and fee to:
Department of Consumer Protection, License Services Division, 165 Capitol Avenue, Hartford, CT 06106
Name of Business (d/ b/ a) |
|
|
|
|
|
FEIN Number: |
|
|
|
|
|
|
|
|
|
Street Address |
|
|
|
City |
|
State |
Zip Code |
|
|
|
|
|
|
|
|
Name of Manager: |
|
Type of Business: |
Telephone Number : |
||||
|
|
|
|
|
|||
Has the Premise had a Previous Non |
|
Name of Previous Businsess & Permit Number: |
|||||
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
||
Name of Parent Company (Corporation, Partnership, LLC, etc.) |
|
|
|
|
|||
|
|
|
|
|
|||
M ailing A ddress (If different than above) |
|
|
|
|
|||
Street Address |
|
|
|
City |
|
State |
Zip Code |
|
|
|
|
|
|
|
|
The applicant understands that in accordance with Section 43(d) of Public Act
*Applicant must return the old permit upon changes in ownership, name or location.
I have read the above statement and understand fully my responsibility as holder of a Non Legend Drug Permit.
_______________________________________________________________ |
_______________________________ |
SIGNATURE OF APPLICANT |
DATE |
|
|