

You'll be able to fill in Form Ps 18 effortlessly with our online PDF tool. We are devoted to giving you the ideal experience with our tool by regularly presenting new features and upgrades. Our editor is now much more intuitive thanks to the most recent updates! At this point, working with documents is simpler and faster than ever. Starting is simple! What you need to do is follow the next easy steps below:
Step 1: Press the "Get Form" button above. It is going to open up our tool so you could start filling in your form.
Step 2: This tool enables you to modify your PDF form in various ways. Improve it by including customized text, adjust what's already in the file, and place in a signature - all within the reach of a couple of clicks!
It's simple to finish the form using out detailed guide! Here's what you should do:
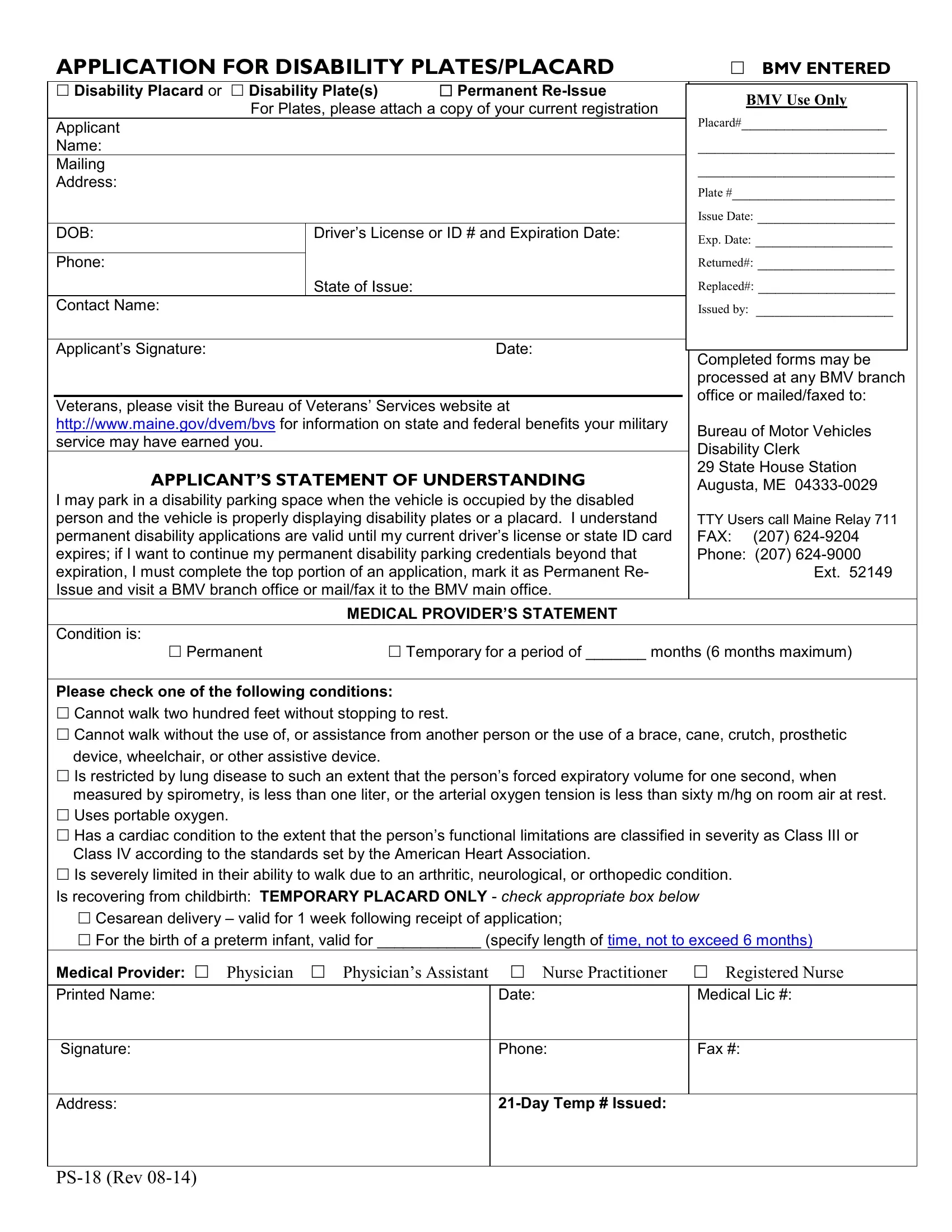
1. The Form Ps 18 requires particular information to be typed in. Be sure that the subsequent blank fields are completed:
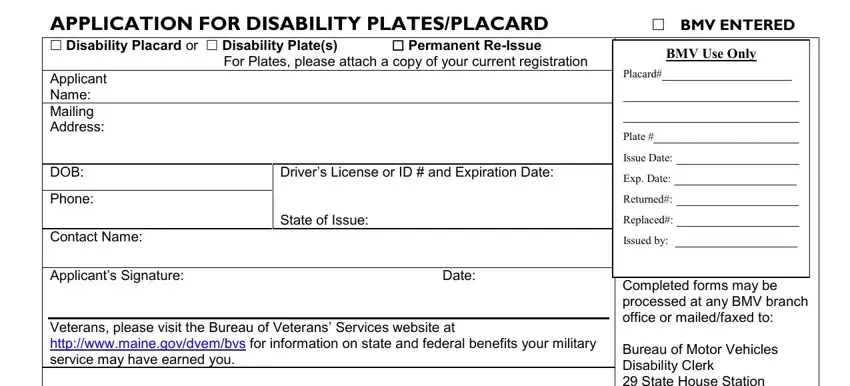
2. The subsequent step is usually to fill in the following fields: MEDICAL PROVIDERS STATEMENT, Condition is Permanent Temporary, Date, Medical Provider Physician, Day Temp Issued, Medical Lic, Phone, and Fax.
Be very mindful while filling out Phone and MEDICAL PROVIDERS STATEMENT, because this is the part in which a lot of people make a few mistakes.
Step 3: Go through what you have inserted in the form fields and press the "Done" button. Get hold of the Form Ps 18 as soon as you subscribe to a free trial. Quickly gain access to the pdf document inside your personal account, with any edits and adjustments being conveniently preserved! We do not sell or share the details that you enter when completing documents at our site.