Every year, the IRS releases a new Form 586-V, which is used to claim the Volunteer Income Tax Assistance (VITA) and Tax Counseling for the Elderly (TCE) programs. This form can be used by individuals or organizations that provide free tax assistance during the filing season. The 2019 version of this form has been released, and it includes several changes that taxpayers should be aware of. In this blog post, we will take a closer look at these changes and discuss how they may impact your tax return. We will also provide tips on how to complete the form accurately. So if you are looking for help filing your taxes this year, be sure to check out our guide to using Form 586-V!
| Question | Answer |
|---|---|
| Form Name | Form Rcoc 586 V |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | 586-V, UCI, RCOC, APS |
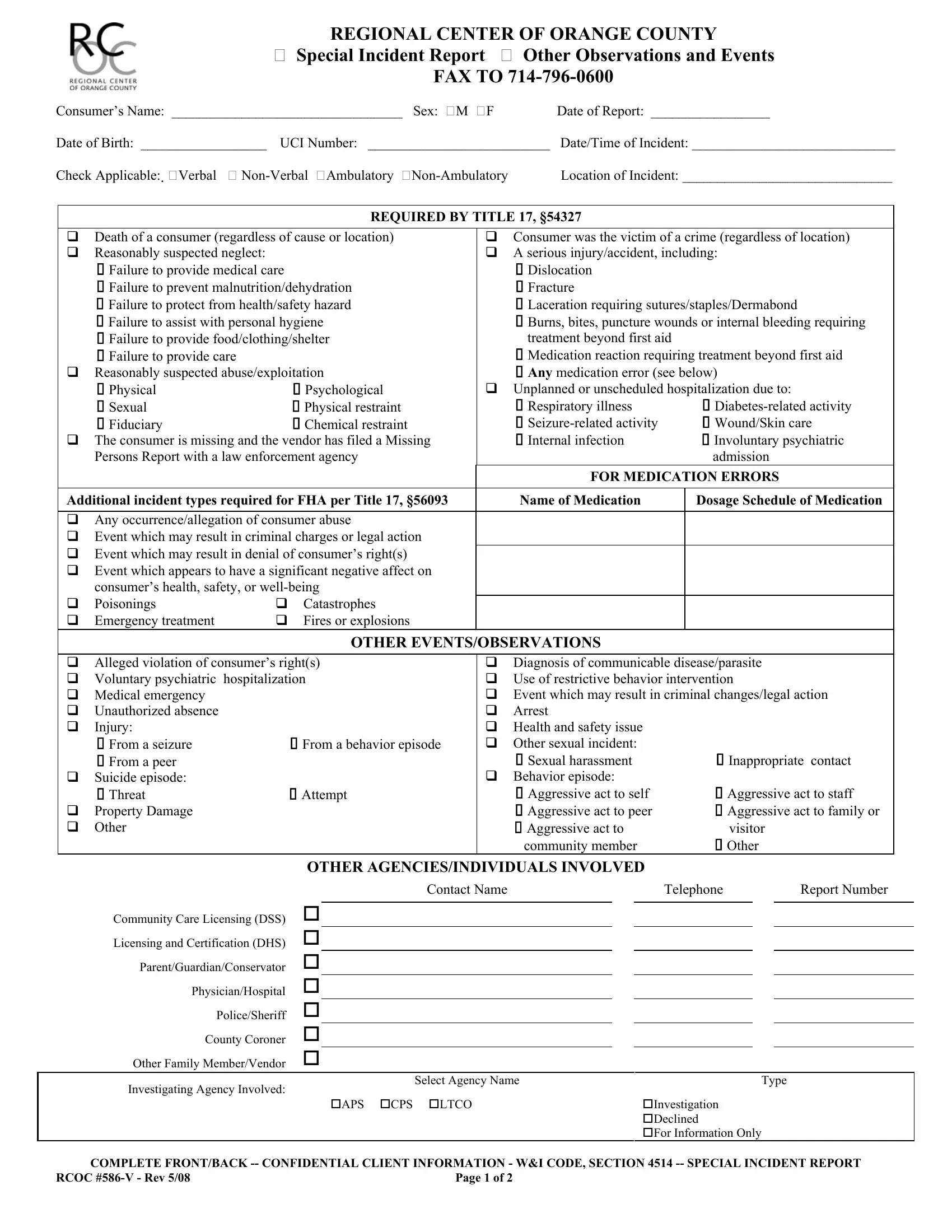
REGIONAL CENTER OF ORANGE COUNTY
Special Incident Report Other Observations and Events
FAX TO
Consumer’s Name: _________________________________ Sex: M F Date of Report: _________________
Date of Birth: __________________ UCI Number: __________________________ Date/Time of Incident: _____________________________
Check Applicable: Verbal |
|
Location of Incident: ______________________________ |
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
REQUIRED BY TITLE 17, §54327 |
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Death of a consumer (regardless of cause or location) |
|
|
|
Consumer was the victim of a crime (regardless of location) |
|
||||||||||
|
Reasonably suspected neglect: |
|
|
|
|
A serious injury/accident, including: |
|
|
||||||||
|
Failure to provide medical care |
|
|
|
|
Dislocation |
|
|
|
|
|
|
||||
|
Failure to prevent malnutrition/dehydration |
|
|
|
|
Fracture |
|
|
|
|
|
|
||||
|
Failure to protect from health/safety hazard |
|
|
|
|
Laceration requiring sutures/staples/Dermabond |
|
|
||||||||
|
Failure to assist with personal hygiene |
|
|
|
|
Burns, bites, puncture wounds or internal bleeding requiring |
|
|||||||||
|
Failure to provide food/clothing/shelter |
|
|
|
|
treatment beyond first aid |
|
|
||||||||
|
Failure to provide care |
|
|
|
|
Medication reaction requiring treatment beyond first aid |
|
|||||||||
|
Reasonably suspected abuse/exploitation |
|
|
|
|
Any medication error (see below) |
|
|
||||||||
|
Physical |
Psychological |
|
|
|
|
Unplanned or unscheduled hospitalization due to: |
|
|
|||||||
|
Sexual |
Physical restraint |
|
|
|
Respiratory illness |
|
|
|
|||||||
|
Fiduciary |
Chemical restraint |
|
|
|
|
|
Wound/Skin care |
|
|||||||
|
The consumer is missing and the vendor has filed a Missing |
|
|
|
Internal infection |
|
Involuntary psychiatric |
|
||||||||
|
Persons Report with a law enforcement agency |
|
|
|
|
|
|
|
|
admission |
|
|
||||
|
|
|
|
|
|
|
|
FOR MEDICATION ERRORS |
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
Additional incident types required for FHA per Title 17, §56093 |
|
Name of Medication |
|
Dosage Schedule of Medication |
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Any occurrence/allegation of consumer abuse |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Event which may result in criminal charges or legal action |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Event which may result in denial of consumer’s right(s) |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Event which appears to have a significant negative affect on |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
consumer’s health, safety, or |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Poisonings |
Catastrophes |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Emergency treatment |
Fires or explosions |
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
OTHER EVENTS/OBSERVATIONS |
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Alleged violation of consumer’s right(s) |
|
|
|
|
Diagnosis of communicable disease/parasite |
|
|
||||||||
|
Voluntary psychiatric |
hospitalization |
|
|
|
|
Use of restrictive behavior intervention |
|
|
|||||||
|
Medical emergency |
|
|
|
|
|
|
Event which may result in criminal changes/legal action |
|
|||||||
|
Unauthorized absence |
|
|
|
|
Arrest |
|
|
|
|
|
|
||||
|
Injury: |
|
|
|
|
|
|
Health and safety issue |
|
|
|
|
|
|
||
|
From a seizure |
From a behavior episode |
|
Other sexual incident: |
|
|
|
|
|
|
||||||
|
From a peer |
|
|
|
|
|
|
Sexual harassment |
|
Inappropriate contact |
|
|||||
|
Suicide episode: |
|
|
|
|
|
|
Behavior episode: |
|
|
|
|
|
|
||
|
Threat |
Attempt |
|
|
|
|
Aggressive act to self |
|
Aggressive act to staff |
|
||||||
|
Property Damage |
|
|
|
|
|
|
Aggressive act to peer |
|
Aggressive act to family or |
|
|||||
|
Other |
|
|
|
|
|
|
Aggressive act to |
|
visitor |
|
|
||||
|
|
|
|
|
|
|
|
community member |
|
Other |
|
|
||||
|
|
OTHER AGENCIES/INDIVIDUALS INVOLVED |
|
|
|
|
|
|
||||||||
|
|
|
|
Contact Name |
|
|
|
Telephone |
Report Number |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Community Care Licensing (DSS) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Licensing and Certification (DHS) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Parent/Guardian/Conservator |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Physician/Hospital |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Police/Sheriff |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
County Coroner |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Other Family Member/Vendor |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|||||||
|
Investigating Agency Involved: |
Select Agency Name |
|
|
Type |
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
APS |
CPS |
LTCO |
|
|
Investigation |
|
|
||||||
|
|
|
|
|
|
|
|
|
|
Declined |
|
|
||||
|
|
|
|
|
|
|
|
|
|
For Information Only |
|
|
||||
|
COMPLETE FRONT/BACK |
|
||||||||||||||
RCOC |
|
|
|
Page 1 of 2 |
|
|
|
|
|
|
|
|
|
|||
DESCRIPTION OF INCIDENT (Title 17 requires a description of the alleged perpetrator, if applicable):
(Attach a separate page for additional information if necessary)
IMMEDIATE ACTION TAKEN BY SERVICE PROVIDER/VENDOR/OTHER:
(Attach a separate page for additional information if necessary)
MEDICAL TREATMENT NECESSARY: Yes No If Yes, Nature of Treatment:
Administered At: ___________________________________ |
Administered By:_____________________________________ |
PLAN TO PREVENT FURTHER OCCURRENCES:
(Attach a separate page for additional information if necessary)
COMMENTS (INCLUDE THE NAME/ADDRESS OF ANY WITNESS TO THE INCIDENT):
(Attach a separate page for additional information if necessary)
|
REPORT SUBMITTED BY |
||
|
|
|
|
Name (print): |
|
Title: |
|
Vendor Name: |
|
Vendor Number: |
|
|
|
||
Telephone Number: |
|
Signature/Date: |
|
COMPLETE FRONT/BACK |
|||
RCOC |
Page 2 of 2 |
||