
You could complete Form Sc Emp5093 effortlessly with the help of our online PDF tool. To maintain our editor on the cutting edge of practicality, we aim to put into practice user-oriented features and enhancements on a regular basis. We are routinely grateful for any feedback - join us in remolding the way you work with PDF forms. Here is what you would want to do to begin:
Step 1: Click on the "Get Form" button at the top of this page to get into our editor.
Step 2: After you launch the file editor, you'll see the form ready to be filled out. Other than filling out different blanks, you may also perform several other actions with the PDF, such as writing your own words, editing the original textual content, inserting graphics, placing your signature to the form, and much more.
This PDF will require specific information to be filled in, thus be sure to take whatever time to fill in exactly what is requested:
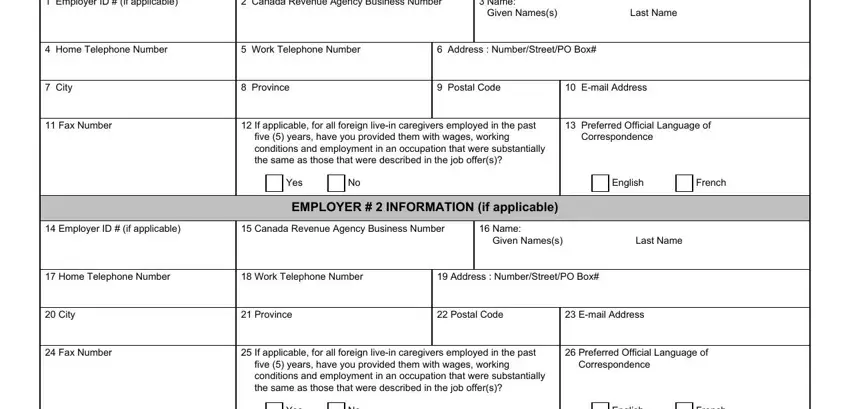
1. You have to complete the Form Sc Emp5093 correctly, so be mindful when filling out the parts including all these fields:
2. After completing the previous section, head on to the subsequent stage and fill out the necessary details in all these blank fields - Given Names, Last Name, Telephone Number, Spouse CommonLawPartner Other, Third Party ID if applicable, Canada Revenue Agency Business, Third Party Business Name, THIRD PARTY INFORMATION if, Third Party Representative, Preferred Official Language of, English, French, Address NumberStreetPO Box, City, and Province.
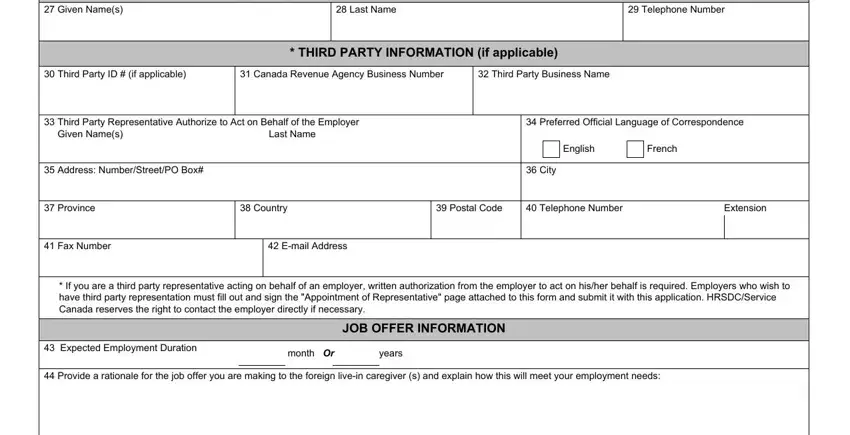
Concerning English and THIRD PARTY INFORMATION if, ensure you get them right in this current part. Those two are certainly the key ones in the document.
3. This next portion is all about Details of individuals to be cared, Child care, Care of elderly person, Care of person with disability, Child care, Care of elderly person, Care of person with disability, Child care, Care of elderly person, Care of person with disability, Child care, Care of elderly person, Care of person with disability, Child care, and Care of elderly person - complete each of these fields.
4. This fourth section comes next with the next few blanks to complete: Language requirements, Oral, English, French, Other, Written, English, French, Other, If Other please explain, Wage in Canadian Dollars and, per hour, per month, Benefits, and Disability insurance.
5. While you come close to the final sections of your document, you'll find a few more things to undertake. Particularly, Have you attempted to recruit, Yes If yes please provide details, If you posted your job offer on, Attach supporting documentation, No If no please explain, Name of Foreign Livein Caregiver, Gender, FOREIGN LIVEIN CAREGIVER, Surname family name as Shown on, Given Names as Shown on the, Male, Female, Date of Birth YYYYMMDD, Location of Residence Outside, and Citizenship must be done.
Step 3: Be certain that your details are correct and press "Done" to continue further. After creating afree trial account at FormsPal, you'll be able to download Form Sc Emp5093 or send it via email without delay. The file will also be accessible through your personal account page with all of your modifications. Here at FormsPal.com, we do everything we can to be certain that your details are maintained protected.