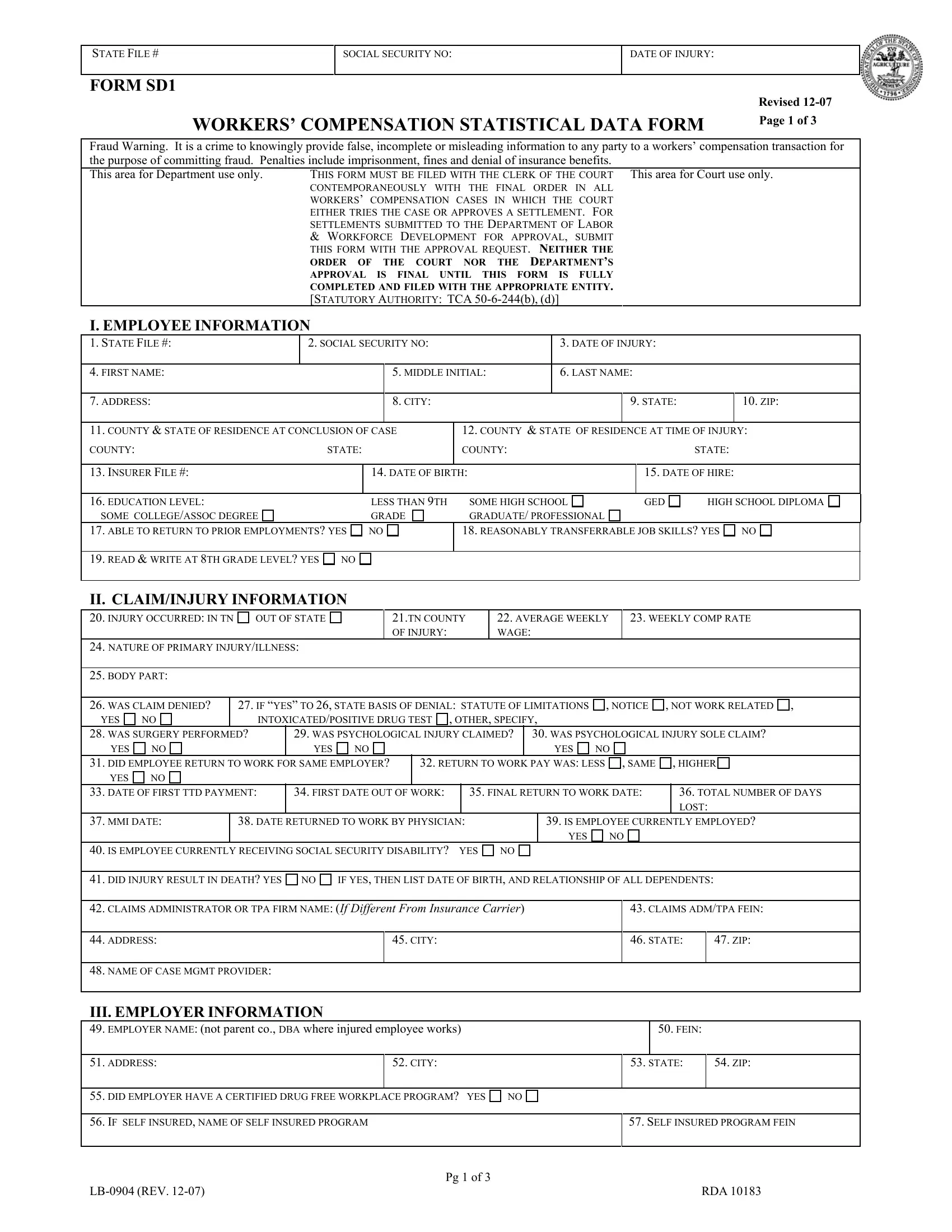
When navigating through the complexities of workers’ compensation claims, the form SD1 stands out as a crucial document that ensures transparency and accuracy in reporting statistical data. Tailored to accompany the final order in workers' compensation cases, whether through a trial or an approved settlement, this form integrates crucial data spanning from employee information, claim specifics, to medical and vocational expert insights. Crafted with the intent to mitigate fraudulent activities, it carries a stern warning against the provision of misleading information, underlining the legal and financial repercussions of such actions. It meticulously collects comprehensive details ranging from personal identifiers like social security numbers to nuanced medical information, including the nature of injuries and the involvement of psychological claims. It also delves into the aftermath of the injury, probing into employment status post-injury, the financial aspects like compensation rates, and the broader implications of the case, including settlements and court approvals. This stringent procedure, mandated for court and Department of Labor and Workforce Development filings, underscores the legal system’s diligence in ensuring that workers’ compensation cases are handled with utmost precision and integrity, ultimately aiming to foster a fair and just resolution for all parties involved.
| Question | Answer |
|---|---|
| Form Name | Form Sd1 |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | WKS, FEIN, SD1, LB-0904 |
STATE FILE #
SOCIAL SECURITY NO:
DATE OF INJURY:
FORM SD1
WORKERS’ COMPENSATION STATISTICAL DATA FORM
Revised
Page 1 of 3
Fraud Warning. It is a crime to knowingly provide false, incomplete or misleading information to any party to a workers’ compensation transaction for the purpose of committing fraud. Penalties include imprisonment, fines and denial of insurance benefits.
This area for Department use only. |
THIS FORM MUST BE FILED WITH THE CLERK OF THE COURT This area for Court use only. |
|
CONTEMPORANEOUSLY WITH THE FINAL ORDER IN ALL |
|
WORKERS’ COMPENSATION CASES IN WHICH THE COURT |
|
EITHER TRIES THE CASE OR APPROVES A SETTLEMENT. FOR |
SETTLEMENTS SUBMITTED TO THE DEPARTMENT OF LABOR
& WORKFORCE DEVELOPMENT FOR APPROVAL, SUBMIT
THIS FORM WITH THE APPROVAL REQUEST. NEITHER THE
ORDER OF THE COURT NOR THE DEPARTMENT’S APPROVAL IS FINAL UNTIL THIS FORM IS FULLY
COMPLETED AND FILED WITH THE APPROPRIATE ENTITY. [STATUTORY AUTHORITY: TCA
I. EMPLOYEE INFORMATION
1. |
STATE FILE #: |
2. SOCIAL SECURITY NO: |
3. |
DATE OF INJURY: |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
4. |
FIRST NAME: |
|
|
5. |
MIDDLE INITIAL: |
6. |
LAST NAME: |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
7. |
ADDRESS: |
|
|
8. |
CITY: |
|
|
9. STATE: |
10. ZIP: |
||
|
|
|
|
|
|
|
|
||||
11. COUNTY & STATE OF RESIDENCE AT CONCLUSION OF CASE |
|
12. COUNTY & STATE OF RESIDENCE AT TIME OF INJURY: |
|||||||||
COUNTY: |
STATE: |
|
COUNTY: |
|
|
|
STATE: |
|
|||
|
|
|
|
|
|
|
|
|
|||
13. INSURER FILE #: |
|
14. DATE OF BIRTH: |
|
|
|
15. DATE OF HIRE: |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
16.EDUCATION LEVEL:
SOME COLLEGE/ASSOC DEGREE
LESS THAN 9TH |
SOME HIGH SCHOOL |
GED |
GRADE |
GRADUATE/ PROFESSIONAL |
|
HIGH SCHOOL DIPLOMA
17. ABLE TO RETURN TO PRIOR EMPLOYMENTS? YES NO
18. REASONABLY TRANSFERRABLE JOB SKILLS? YES NO
19.READ & WRITE AT 8TH GRADE LEVEL? YES NO
II. CLAIM/INJURY INFORMATION
20. INJURY OCCURRED: IN TN |
OUT OF STATE |
|
|
21.TN COUNTY |
22. AVERAGE WEEKLY |
|
23. WEEKLY COMP RATE |
||||||||||||||
|
|
|
|
|
|
|
|
OF INJURY: |
|
|
WAGE: |
|
|
|
|
|
|
|
|||
24. NATURE OF PRIMARY INJURY/ILLNESS: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
25. |
BODY PART: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
26. |
WAS CLAIM DENIED? |
|
27. IF “YES” TO 26, STATE BASIS OF DENIAL: STATUTE OF LIMITATIONS |
, NOTICE |
, NOT WORK RELATED , |
||||||||||||||||
YES |
NO |
|
INTOXICATED/POSITIVE DRUG TEST |
, OTHER, SPECIFY, |
|
|
|
|
|
|
|
||||||||||
28. WAS SURGERY PERFORMED? |
29. WAS PSYCHOLOGICAL INJURY CLAIMED? |
30. WAS PSYCHOLOGICAL INJURY SOLE CLAIM? |
|||||||||||||||||||
|
YES |
NO |
|
YES |
NO |
|
|
|
|
|
|
YES |
NO |
|
|
|
|
||||
31. |
DID EMPLOYEE RETURN TO WORK FOR SAME EMPLOYER? |
|
32. RETURN TO WORK PAY WAS: LESS |
|
, SAME |
|
, HIGHER |
||||||||||||||
|
YES |
NO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
33. |
DATE OF FIRST TTD PAYMENT: |
34. FIRST DATE OUT OF WORK: |
|
35. FINAL RETURN TO WORK DATE: |
|
36. TOTAL NUMBER OF DAYS |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LOST: |
|
|
37. |
MMI DATE: |
|
38. DATE RETURNED TO WORK BY PHYSICIAN: |
|
|
39. IS EMPLOYEE CURRENTLY EMPLOYED? |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
YES |
|
NO |
|
|
|
|
|
40. IS EMPLOYEE CURRENTLY RECEIVING SOCIAL SECURITY DISABILITY? |
YES |
NO |
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
||||||||||||||||
41. |
DID INJURY RESULT IN DEATH? YES |
NO |
IF YES, THEN LIST DATE OF BIRTH, AND RELATIONSHIP OF ALL DEPENDENTS: |
|
|||||||||||||||||
|
|
|
|
|
|
||||||||||||||||
42. |
CLAIMS ADMINISTRATOR OR TPA FIRM NAME: (If Different From Insurance Carrier) |
|
|
43. CLAIMS ADM/TPA FEIN: |
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
44. |
ADDRESS: |
|
|
|
|
45. CITY: |
|
|
|
|
|
|
|
46. STATE: |
|
47. ZIP: |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
48. |
NAME OF CASE MGMT PROVIDER: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
III. EMPLOYER INFORMATION
49. EMPLOYER NAME: (not parent co., DBA where injured employee works) |
|
|
50. FEIN: |
|||
|
|
|
|
|
|
|
51. ADDRESS: |
52. CITY: |
|
53. STATE: |
|
54. ZIP: |
|
|
|
|
|
|
|
|
55. DID EMPLOYER HAVE A CERTIFIED DRUG FREE WORKPLACE PROGRAM? YES |
NO |
|
|
|||
|
|
|
|
|||
56. IF SELF INSURED, NAME OF SELF INSURED PROGRAM |
|
|
57. SELF INSURED PROGRAM FEIN |
|||
|
|
|
|
|
|
|
|
Pg 1 of 3 |
|
|
|
|
|
|
|
|
|
RDA 10183 |
||
STATE FILE #
SOCIAL SECURITY NO:
DATE OF INJURY:
FORM SD1
58.NAME OF INSURANCE CARRIER:
59.INSURANCE CARRIER FEIN:
60.ADDRESS:
61.CITY:
62. STATE: |
63. ZIP: |
|
|
IV. MEDICAL AND VOCATIONAL EXPERTS
NAMES OF TREATING PHYSICIANS
64. |
|
(A) LAST NAME: |
(B) FIRST |
|
(C) MI: |
(D) TITLE: |
|
|
(E) LICENSE NUMBER: |
|
|
|
NAME: |
|
|
MD |
DO |
DC |
|
|
|
(F) IMPAIRMENT RATING (%) |
(G) TO BODY OR SPECIFIC |
(H) SCHEDULED MEMBER LOCATION |
|||||
|
|
|
MEMBER: |
|
|
LEFT |
RIGHT |
|
|
|
|
(A) LAST NAME: |
(B) FIRST |
|
(C) MI: |
(D) TITLE: |
|
|
(E) LICENSE NUMBER: |
|
|
|
NAME: |
|
|
MD |
DO |
DC |
|
|
|
(F) IMPAIRMENT RATING (%) |
(G) TO BODY OR SPECIFIC |
(H) SCHEDULED MEMBER LOCATION |
|||||
|
|
|
MEMBER: |
|
|
LEFT |
RIGHT |
|
|
EMPLOYEE’S IME(s) |
|
|
|
|
|
|
|
||
65. |
|
(A) LAST NAME: |
(B) FIRST |
|
(C) MI: |
(D) TITLE: |
|
|
(E) LICENSE NUMBER: |
|
|
|
NAME: |
|
|
MD |
DO |
DC |
|
|
|
(F) IMPAIRMENT RATING (%) |
(G) TO BODY OR SPECIFIC |
(H) SCHEDULED MEMBER LOCATION |
|||||
|
|
|
MEMBER: |
|
|
LEFT |
RIGHT |
|
|
EMPLOYER’S IME(s) |
|
|
|
|
|
|
|
||
66. |
|
(A) LAST NAME: |
(B) FIRST |
|
(C) MI: |
(D) TITLE: |
|
|
(E) LICENSE NUMBER: |
|
|
|
NAME: |
|
|
MD |
DO |
DC |
|
|
|
(F) IMPAIRMENT RATING (%) |
(G) TO BODY OR SPECIFIC |
(H) SCHEDULED MEMBER LOCATION |
|||||
|
|
|
MEMBER: |
|
|
LEFT |
RIGHT |
|
|
EMPLOYEE’S VOCATIONAL EXPERT |
|
|
|
|
|
|
|
||
67. |
|
(A) LAST NAME: |
(B) FIRST |
|
(C) MI: |
(D) TITLE: |
|
|
(E) VOCATIONAL DISABILITY |
|
|
|
NAME: |
|
|
PHD |
MA |
OTHER |
RATING: |
EMPLOYER’S VOCATIONAL EXPERT |
|
|
|
|
|
|
|
||
68. |
|
(A) LAST NAME: |
(B) FIRST |
|
(C) MI: |
(D) TITLE: |
|
|
(E) VOCATIONAL DISABILITY |
|
|
|
NAME: |
|
|
PHD |
MA |
OTHER |
RATING: |
CHIROPRACTIC/PHYSICAL THERAPY |
|
|
|
|
|
|
|
||
69. CHIROPRACTIC TREATMENT? YES NO |
|
70. PHYSICIAL THERAPY? YES |
NO |
|
|||||
|
IF YES, NUMBER OF VISITS? |
|
|
IF YES, NUMBER OF VISITS? |
|
|
|||
V. TYPE OF CONCLUSION AND COURT IDENTIFICATION INFORMATION
TRIAL (Applicable only when the case has been TRIED by the court.)
SETTLEMENT APPROVED BY COURT
SETTLEMENT APPROVED BY COURT - COMPLAINT NOT FILED. (Applicable only when a lawsuit has NOT been initiated by the filing of a complaint – term “joint petition” used to refer to this type of procedure for purposes of this form.)
71.STYLE OF CASE:
72.COURT DOCKET NO:
73.COUNTY:
74.COURT:
75.FULL NAME OF TRIAL JUDGE/CHANCELLOR:
76.DATE COMPLAINT FILED:
77.DATE OF TRIAL:
78.DATE JOINT PETITION FILED:
79.DATE OF SETTLEMENT APPROVAL:
80.NAME OF APPROVING JUDGE/CHANCELLOR
SETTLEMENT APPROVED BY DEPARTMENT OF LABOR & WORKFORCE DEVELOPMENT (Applicable only when the approval is by the Department.)
81.DATE OF SETTLEMENT APPROVAL BY SPECIALIST:
82.NAME OF SPECIALIST APPROVING SETTLEMENT:
VI. BENEFIT REVIEW CONFERENCE
83.DATE OF CONFERENCE:
84.SETTLED? YES NO
85.NAME OF SPECIALIST:
VII. TRIAL RESULTS
86. PPD% |
|
|
TO BODY OR SPECIFIC MEMBER: |
|
LEFT RIGHT |
||
YES |
NO |
IF YES, NUMBER OF WEEKS? |
|
|
|
|
|
|
|
|
|
|
|
|
|
87. PTD? |
|
|
|
88. DEATH CLAIM? YES |
NO |
||
YES |
NO |
IF YES, NUMBER OF WEEKS? |
|
|
|
|
|
|
|
|
|||||
89. JUDGMENT FOR EMPLOYER? YES NO |
, SELECT BASIS: STATUE OF LIMITATIONS ; NOTICE ; NOT WORK RELATED ; |
||||||
|
NO PERMANENCY ; INTOXICATION |
; WILLFUL MISCONDUCT ; OTHER, SPECIFY |
|
|
|||
|
|
|
|
|
|
||
|
|
|
Pg 2 of 3 |
|
|
||
|
|
|
RDA 10183 |
||||
STATE FILE #
SOCIAL SECURITY NO:
DATE OF INJURY:
FORM SD1
VIII. SETTLEMENT TERMS
90.PPD%
YES NO IF YES, NUMBER OF WEEKS?
TO BODY OR SPECIFIC MEMBER:
LEFT
RIGHT
91. PTD? |
|
|
|
92. DEATH CLAIM? YES NO |
YES NO |
IF YES, NUMBER OF WEEKS? |
|
|
|
|
|
|
|
|
93. FUTURE MEDICAL EXPENSE: CLOSED ; OPEN FOR LIFE |
; OR, OPEN FOR A SPECIFIED PERIOD? |
|||
|
|
|
||
94. WAS MONEY PAID TO CLOSE FUTURE MEDICALS? |
|
95. DATE MEDICALS WERE OR WILL BE CLOSED: |
||
YES |
NO |
|
|
|
|
|
|
||
96. WAS CASE SETTLED PURSUANT TO TCA |
YES NO |
|||
IX. SECOND INJURY FUND
97. IS THIS A SECOND INJURY FUND CLAIM? |
98. WAS JUDGMENT ENTERED AGAINST SECOND INJURY FUND? |
|||
YES NO |
|
YES |
NO |
|
|
|
|
|
|
99. APPORTIONMENT: |
(1) EMPLOYER; ____ %; #WKS; __________TOTAL AMT. |
|
(2) SECOND INJ FUND ____ %; #WKS; _________ TOTAL AMT. |
|
|
|
|
|
|
X. MONETARY AMOUNTS PAID
TYPE OF BENEFIT |
PAID PRIOR TO TRIAL/ |
PAID PURSUANT TO TRIAL |
PAID PURSUANT TO |
TOTAL PAYMENTS |
|
SETTLEMENT |
RESULTS |
SETTLEMENT TERMS |
|
100.TEMP TOTAL DISABILITY
101.TEMP PARTIAL DISABILITY
102.PERMANENT PARTIAL DISABILITY
103.PERMANENT TOTAL DISABILITY
104.DEATH BENEFITS
105.BURIAL EXPENSES
106.MEDICAL EXPENSES TOTAL
(includes medicine, PT, chiro, hospital, |
|
|||
MD/DO costs, tests) |
|
|||
107. CASE MANAGEMENT COSTS |
|
|||
|
|
|
|
|
108. DISCRETIONARY COSTS |
|
|||
|
|
|
|
|
109. AMOUNT PAID TO CLOSE FUTURE MEDICAL EXPENSE |
|
|||
|
|
|
|
|
110. LUMP SUM PAYMENT (not based on specific disability %) |
|
|||
|
|
|
|
|
111 DATE LUMP SUM PAID (not based on specific disability %): ______________________ |
|
|||
|
|
|
|
|
112. TOTALS (ADD TOTALS FROM LINES 100 THRU 110) |
|
|
|
|
|
|
|
|
|
113. AMOUNT PAID IN LUMP SUM FROM LINES 100 THRU 105; _________________________ |
114. DATE LUMP SUM PAID FROM LINES 100 |
|||
(DO NOT ADD THIS AMOUNT TO TOTAL PAYMENTS. IT IS ALREADY INCLUDED IN THE TOTALS ABOVE.) |
THRU 105 ___________________ |
|||
|
|
|
||
XI. ATTORNEYS FEES |
|
|||
115. EMPLOYEE’S ATTORNEY FEE; |
|
116. WAS FEE APPROVED BY COURT |
||
AMOUNT OF AWARD ______________ % OF AWARD __________ |
|
OR TDLWD |
||
117. EMPLOYER’S ATTORNEY FEE (SPECIFY RANGE): UNDER $1500 ; |
; OVER $10,000 |
|||
|
|
|
||
XII. |
CERTIFICATION AND SIGNATURES |
|
||
By providing my BPR number and my signature, I hereby certify that I have read the contents of the form and the information provided is true and correct to the best of my knowledge. ATTORNEY MUST PROVIDE BPR# .
118. NAME OF EMPLOYEE’S ATTORNEY: |
BPR# |
119. NAME OF EMPLOYER’S ATTORNEY: |
BPR# |
120.NAME OF EMPLOYEE:
121.NAME OF ADJUSTER/CARRIER/EMPLOYER REPRESENTATIVE:
SIGNATURE OF EMPLOYEE |
DATE |
SIGNATURE OF ADJUSTER/CARRIER/EMPLOYER REP |
DATE SIGNED |
|
|
SIGNED |
|
|
|
|
|
|
|
|
SIGNATURE OF EMPLOYEE’S ATTORNEY |
DATE |
SIGNATURE OF EMPLOYER’S ATTORNEY |
DATE SIGNED |
|
|
SIGNED |
|
|
|
|
Pg 3 of 3 |
|
|
|
|
|
RDA 10183 |
|
|