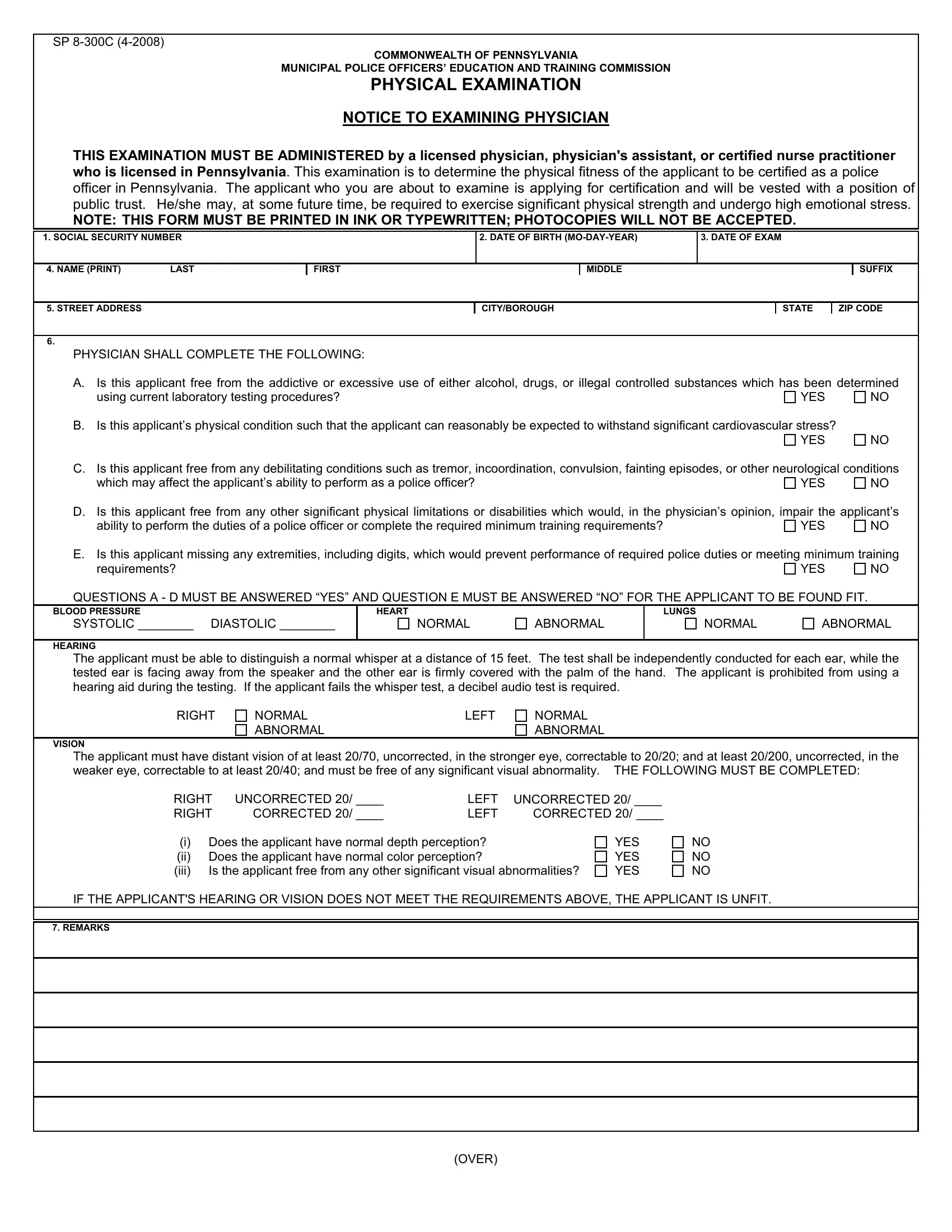
The SP 8-300C form, issued by the Commonwealth of Pennsylvania, plays a critical role in assessing the physical readiness of individuals aiming to become certified police officers within the state. Enforcing stringent criteria, this document mandates a comprehensive examination by a licensed physician, physician's assistant, or a certified nurse practitioner, ensuring applicants meet health standards crucial for the demands of law enforcement duties. The form meticulously evaluates an applicant's freedom from addictive substances, ability to withstand cardiovascular stress, absence of debilitating conditions, and other significant physical or sensory impairments that might hinder police work. Key elements such as blood pressure, heart and lung function, hearing, and vision are scrutinized, with specific benchmarks set for each to determine an applicant's fitness. Notably, aspects like unaided vision, depth perception, color perception, and hearing capabilities without aids are examined, reflecting the rigorous physical and sensory demands placed on police officers. Additionally, the form underscores the importance of truthfulness and legal accountability, requiring signed attestations from both the examiner and the applicant regarding the accuracy of provided information, emphasizing the gravity of the certification process in maintaining high standards for public safety roles.
| Question | Answer |
|---|---|
| Form Name | Form Sp 8 300C |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | aforesaid, designee, UNSWORN, BORO |
SP
COMMONWEALTH OF PENNSYLVANIA
MUNICIPAL POLICE OFFICERS’ EDUCATION AND TRAINING COMMISSION
PHYSICAL EXAMINATION
NOTICE TO EXAMINING PHYSICIAN
THIS EXAMINATION MUST BE ADMINISTERED by a licenSed physician, physician's assistant, or certified nurse practitioner who is licensed in Pennsylvania. This examination is to determine the physical fitness of the applicant to be certified as a police officer in Pennsylvania. The applicant who you are about to examine is applying for certification and will be vested with a position of public trust. He/she may, at some future time, be required to exercise significant physical strength and undergo high emotional stress.
NOTE: THIS FORM MUST BE PRINTED IN INK OR TYPEWRITTEN; PHOTOCOPIES WILL NOT BE ACCEPTED.
1. SOCIAL SECURITY NUMBER
2. DATE OF BIRTH
3. DATE OF EXAM
4. NAME (PRINT) |
LAST |
FIRST
MIDDLE
SUFFIX
5. STREET ADDRESS
CITY/BOROUGH
STATE |
ZIP CODE |
6.
PHYSICIAN SHALL COMPLETE THE FOLLOWING:
A. Is this applicant free from the addictive or excessive use of either alcohol, drugs, or illegal controlled substances which has been determined
using current laboratory testing procedures? |
YES |
NO |
B.Is this applicant’s physical condition such that the applicant can reasonably be expected to withstand significant cardiovascular stress?
YES
NO
C. |
Is this applicant free from any debilitating conditions such as tremor, incoordination, convulsion, fainting episodes, or other neurological conditions |
||
|
which may affect the applicant’s ability to perform as a police officer? |
YES |
NO |
D. |
Is this applicant free from any other significant physical limitations or disabilities which would, in the physician’s opinion, impair the applicant’s |
||
|
ability to perform the duties of a police officer or complete the required minimum training requirements? |
YES |
NO |
E. |
Is this applicant missing any extremities, including digits, which would prevent performance of required police duties or meeting minimum training |
||
|
requirements? |
YES |
NO |
QUESTIONS A - D MUST BE ANSWERED “YES” AND QUESTION E MUST BE ANSWERED “NO” FOR THE APPLICANT TO BE FOUND FIT.
BLOOD PRESSURE
SYSTOLIC ________ DIASTOLIC ________
HEART
NORMAL
ABNORMAL
LUNGS
NORMAL
ABNORMAL
HEARING
The applicant must be able to distinguish a normal whisper at a distance of 15 feet. The test shall be independently conducted for each ear, while the tested ear is facing away from the speaker and the other ear is firmly covered with the palm of the hand. The applicant is prohibited from using a hearing aid during the testing. If the applicant fails the whisper test, a decibel audio test is required.
RIGHT
NORMAL |
LEFT |
ABNORMAL |
|
NORMAL ABNORMAL
VISION
The applicant must have distant vision of at least 20/70, uncorrected, in the stronger eye, correctable to 20/20; and at least 20/200, uncorrected, in the weaker eye, correctable to at least 20/40; and must be free of any significant visual abnormality. THE FOLLOWING MUST BE COMPLETED:
RIGHT |
UNCORRECTED 20/ ____ |
LEFT |
UNCORRECTED 20/ ____ |
||
RIGHT |
CORRECTED 20/ ____ |
LEFT |
CORRECTED 20/ ____ |
||
(i) |
Does the applicant have normal depth perception? |
|
YES |
||
(ii) |
Does the applicant have normal color perception? |
|
YES |
||
(iii) |
Is the applicant free from any other significant visual abnormalities? |
YES |
|||
NO NO NO
IF THE APPLICANT'S HEARING OR VISION DOES NOT MEET THE REQUIREMENTS ABOVE, THE APPLICANT IS UNFIT.
7. REMARKS
(OVER)
8.
PHYSICAL CERTIFICATION
I HAVE PERSONALLY EXAMINED THE ABOVE- NAMED APPLICANT, AND IT IS MY PROFESSIONAL OPINION THAT THIS PERSON IS PHYSICALLY FIT OR UNFIT TO BE CERTIFIED AS A POLICE OFFICER IN PENNSYLVANIA AS INDICATED BELOW:
PHYSICAL VERIFICATION
I HEREBY CERTIFY THAT THE INFORMATION AND STATEMENTS CONTAINED IN THIS EXAMINATION FORM ARE TRUE AND CORRECT, AND THAT I AM SIGNING THIS DOCUMENT WITH THE FULL UNDERSTANDING THAT ANY FALSE INFORMATION OR STATEMENT WILL SUBJECT ME TO CRIMINAL PENALTIES OF 18 PA.C.S. § 4904, RELATING TO UNSWORN FALSIFICATION TO AUTHORITIES.
FIT |
UNFIT ____________________ |
_______________________________________________ |
||
|
DATE |
SIGNATURE - EXAMINING PHYSICIAN |
|
|
|
|
|
|
|
A. NAME OF EXAMINING PHYSICIAN (PRINT) |
|
B. LICENSE NO. |
C. STATE |
|
|
|
|
|
|
D. STREET ADDRESS
CITY/BORO
STATE |
ZIP CODE |
E. TELEPHONE NO. |
|
|
|
- |
- |
|
|
|
|
9.
RELEASE OF PHYSICAL INFORMATION
Having applied for certification as a police officer in Pennsylvania I, ________________________________________________ , have duly subjected
NAME OF APPLICANT
myself to a physical examination by _________________________________________________________ , as required by the Act. I hereby reserve
NAME OF PHYSICIAN
the right to have the data and conclusions of the physician remain confidential except to those whom I designate.
I hereby grant release for the aforesaid information to the police department employing me and the Municipal Police Officers’ Education and Training Commission, or official designee, for purposes consistent with the application process pursuant to this Act. No other release of this information, explicit or implied, is granted at this time.
__________________________________________________ |
______________________________________________ |
__________________ |
|
SIGNATURE - APPLICANT |
SOCIAL SECURITY NO. |
SIGNATURE - EXAMINING PHYSICIAN |
DATE |
FORM PROCESSING
This examination form must be forwarded to the employing police department by the examining physician within 15 days of the date of examination, even if the applicant is found unfit, and forwarded by that department with an application for certification to the Municipal Police Officers’ Education and Training Commission.