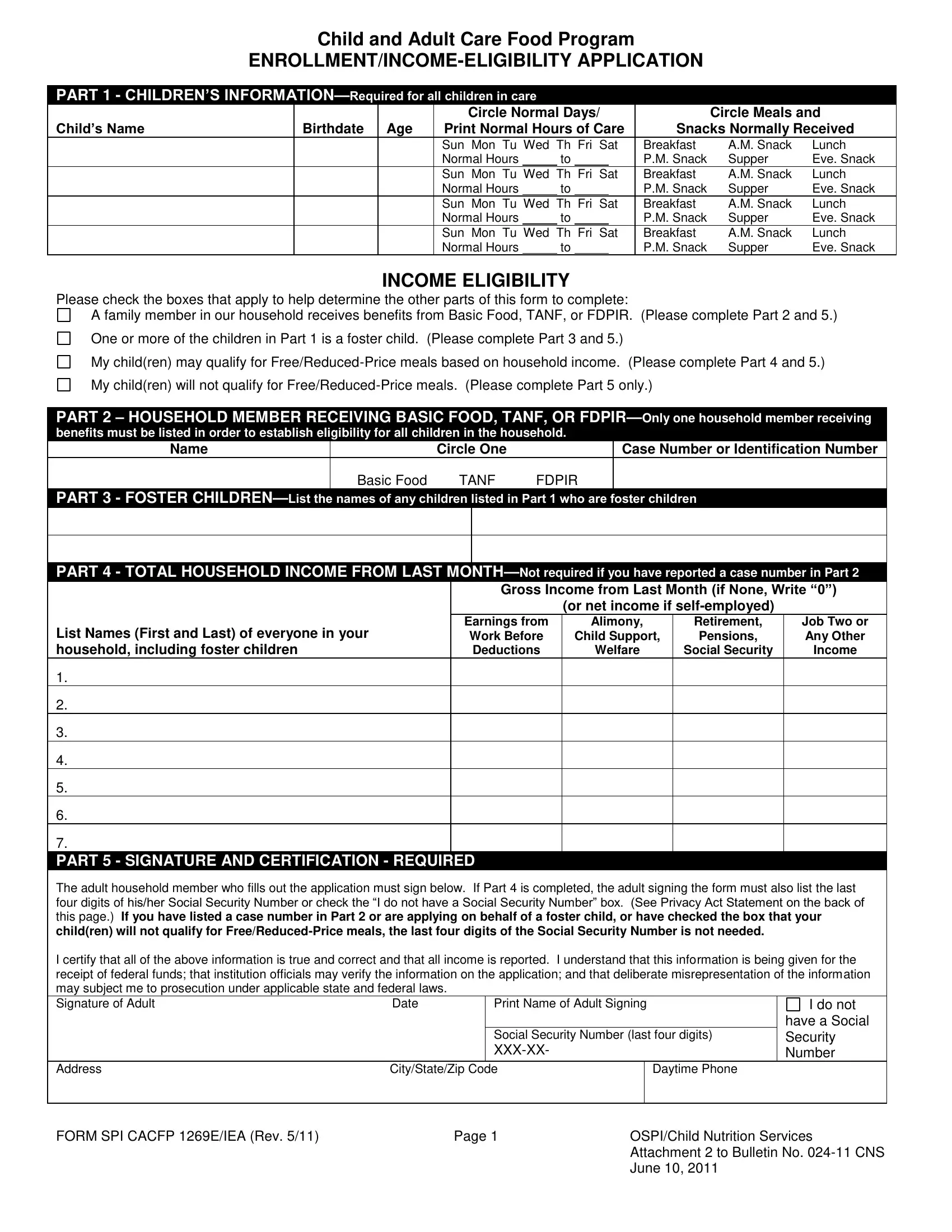
Navigating the complexities of child and adult care food programs can be challenging, but the SPI CACFP 1269E IEA form serves as a critical tool in this process. Designed to streamline the enrollment and income eligibility application for food assistance, this form captures essential information spanning from child details to household income, enabling families and care providers to secure the necessary support efficiently. Key sections include detailed child information such as name, birthdate, days and hours of care alongside meals and snacks received, which ensures that the nutritional needs of children in care are thoroughly documented and met. It also delves into household income eligibility, fostering a clear pathway for determining assistance levels. By including areas to list household members receiving benefits like Basic Food, TANF, or FDPIR, and specifying if any of the children are foster children, the form comprehensively covers various scenarios that could affect eligibility and categorization. A pivotal component of the form is the signature and certification part, underscoring the applicant's responsibility to provide true and accurate information under the guidance of state and federal laws. Additionally, it touches on sensitive areas such as the Social Security Number requirement, with clear indications for when these details are mandatory or when exemptions apply, all underscored by the Privacy Act Statement which highlights the lawful use of this information. Through this form, applicants are also encouraged to voluntarily provide children's ethnic and racial identities to ensure equitable access and address any discrimination concerns, further emphasizing the program's commitment to fairness and inclusivity.
| Question | Answer |
|---|---|
| Form Name | Form Spi Cacfp 1269E Iea |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | 2011, FDPIR, TANF, CACFP |
Child and Adult Care Food Program
PART 1 - CHILDREN’S
Child’s Name |
|
Circle Normal Days/ |
|
Circle Meals and |
|||||
Birthdate Age |
Print Normal Hours of Care |
Snacks Normally Received |
|||||||
|
|
Sun Mon Tu Wed Th Fri Sat |
Breakfast |
A.M. Snack |
Lunch |
||||
|
|
Normal Hours |
|
to |
P.M. Snack |
Supper |
Eve. Snack |
||
|
|
|
|
|
|
||||
|
|
Sun Mon Tu Wed Th Fri Sat |
Breakfast |
A.M. Snack |
Lunch |
||||
|
|
Normal Hours |
|
to |
P.M. Snack |
Supper |
Eve. Snack |
||
|
|
Sun Mon Tu Wed Th Fri Sat |
Breakfast |
A.M. Snack |
Lunch |
||||
|
|
Normal Hours |
|
to |
P.M. Snack |
Supper |
Eve. Snack |
||
|
|
Sun Mon Tu Wed Th Fri Sat |
Breakfast |
A.M. Snack |
Lunch |
||||
|
|
Normal Hours |
|
to |
|
|
P.M. Snack |
Supper |
Eve. Snack |
INCOME ELIGIBILITY
Please check the boxes that apply to help determine the other parts of this form to complete:
A family member in our household receives benefits from Basic Food, TANF, or FDPIR. (Please complete Part 2 and 5.)
One or more of the children in Part 1 is a foster child. (Please complete Part 3 and 5.)
My child(ren) may qualify for
My child(ren) will not qualify for
PART 2 – HOUSEHOLD MEMBER RECEIVING BASIC FOOD, TANF, OR
benefits must be listed in order to establish eligibility for all children in the household.
Name |
Circle One |
Case Number or Identification Number |
Basic Food |
TANF |
FDPIR |
PART 3 - FOSTER
PART 4 - TOTAL HOUSEHOLD INCOME FROM LAST
(or net income if
List Names (First and Last) of everyone in your |
Earnings from |
Alimony, |
Retirement, |
Job Two or |
Work Before |
Child Support, |
Pensions, |
Any Other |
|
household, including foster children |
Deductions |
Welfare |
Social Security |
Income |
1.
2.
3.
4.
5.
6.
7.
PART 5 - SIGNATURE AND CERTIFICATION - REQUIRED
The adult household member who fills out the application must sign below. If Part 4 is completed, the adult signing the form must also list the last four digits of his/her Social Security Number or check the “I do not have a Social Security Number” box. (See Privacy Act Statement on the back of
this page.) If you have listed a case number in Part 2 or are applying on behalf of a foster child, or have checked the box that your child(ren) will not qualify for
I certify that all of the above information is true and correct and that all income is reported. I understand that this information is being given for the receipt of federal funds; that institution officials may verify the information on the application; and that deliberate misrepresentation of the information may subject me to prosecution under applicable state and federal laws.
Signature of Adult |
Date |
Print Name of Adult Signing |
I do not |
|
|
|
have a Social |
|
|
Social Security Number (last four digits) |
Security |
|
|
Number |
Address |
City/State/Zip Code |
Daytime Phone
FORM SPI CACFP 1269E/IEA (Rev. 5/11) |
Page 1 |
OSPI/Child Nutrition Services |
|
|
Attachment 2 to Bulletin No. |
|
|
June 10, 2011 |
PART 6 – CHILDREN’S ETHNIC AND RACIAL
Check the ethnic and racial category of your child. We need this information to be sure that everyone receives benefits on a fair basis.
Ethnicity: |
|
Hispanic or Latino |
No child will be discriminated against because of race, |
Not Hispanic or Latino |
color, national origin, gender, age, or disability. |
Race: |
|
White |
|
Black or African American |
|
Asian |
|
American Indian or Alaskan Native |
|
Native Hawaiian or Pacific Islander |
|
|
If you feel you have been discriminated against, you should write USDA, Director of Civil Rights, 1400 Independence Avenue SW, Washington, DC
PRIVACY ACT STATEMENT
The Richard B. Russell National School Lunch Act requires that, unless a household member’s Basic Food, TANF, or FDPIR case number is provided or you are applying on behalf of a foster child, you must include the last four digits of the Social Security Number of the adult household member signing the application, or indicate that the household member does not have a Social Security Number. Provision of the last four digits of the Social Security Number is not mandatory, but if the last four digits of the Social Security Number is not provided or an indication is not made that the signer does not have a Social Security Number, the application cannot be approved in the free or
CENTER USE ONLY
Foster child(ren) have been identified on this form and qualify for the free category.
Child(ren) on this form who are not foster children qualify as follows:
Check one:
Free Category |
|
|
|
Total Monthly Income $ |
This form must be signed and dated by the institution’s representative.
|
Signature of Institution’s Representative |
|
Date |
|
|
|
|
|
|
FORM SPI CACFP 1269E/IEA (Rev. 5/11) |
Page 2 |
OSPI/Child Nutrition Services |
|
|
Attachment 2 to Bulletin No. |
|
|
June 10, 2011 |