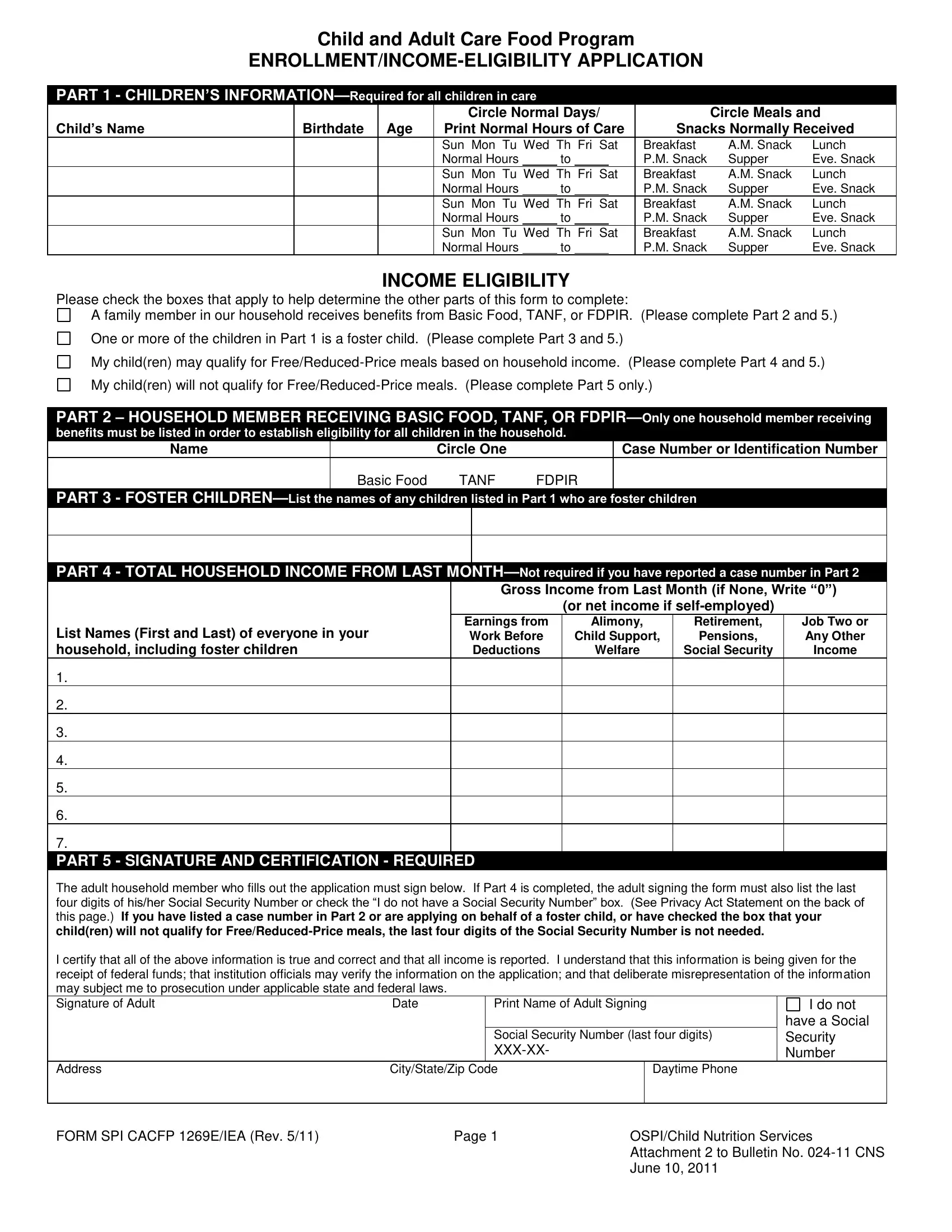
Navigating the complexities of child and adult care food programs can be challenging, but the SPI CACFP 1269E IEA form serves as a critical tool in this process. Designed to streamline the enrollment and income eligibility application for food assistance, this form captures essential information spanning from child details to household income, enabling families and care providers to secure the necessary support efficiently. Key sections include detailed child information such as name, birthdate, days and hours of care alongside meals and snacks received, which ensures that the nutritional needs of children in care are thoroughly documented and met. It also delves into household income eligibility, fostering a clear pathway for determining assistance levels. By including areas to list household members receiving benefits like Basic Food, TANF, or FDPIR, and specifying if any of the children are foster children, the form comprehensively covers various scenarios that could affect eligibility and categorization. A pivotal component of the form is the signature and certification part, underscoring the applicant's responsibility to provide true and accurate information under the guidance of state and federal laws. Additionally, it touches on sensitive areas such as the Social Security Number requirement, with clear indications for when these details are mandatory or when exemptions apply, all underscored by the Privacy Act Statement which highlights the lawful use of this information. Through this form, applicants are also encouraged to voluntarily provide children's ethnic and racial identities to ensure equitable access and address any discrimination concerns, further emphasizing the program's commitment to fairness and inclusivity.
| Question | Answer |
|---|---|
| Form Name | Form Spi Cacfp 1269E Iea |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | 2011, FDPIR, TANF, CACFP |