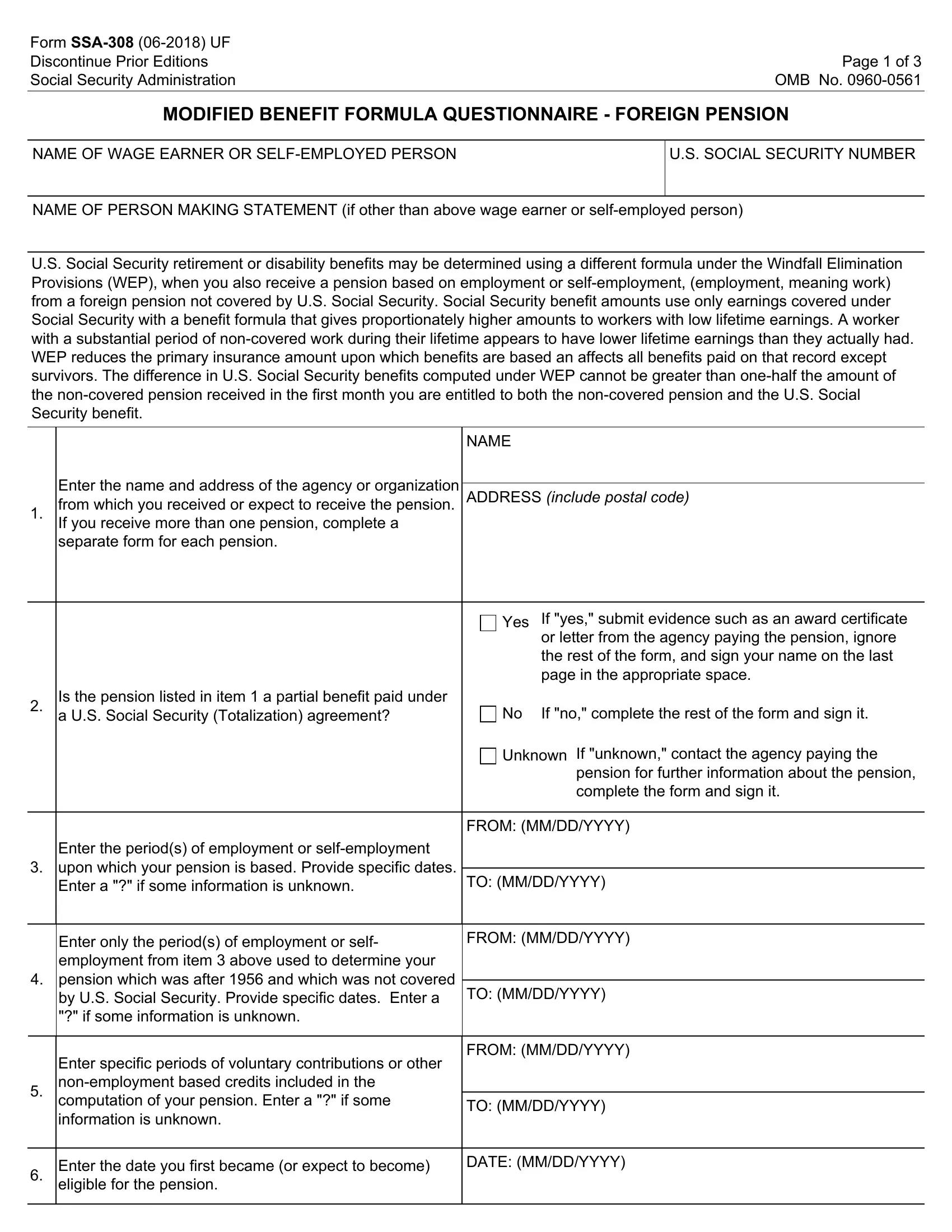
The Form SSA-308 serves a crucial role for individuals receiving pensions from foreign employment not covered by U.S. Social Security, potentially triggering an adjustment to their U.S. Social Security benefits under the Windfall Elimination Provision (WEP). The purpose of this form is to gather detailed information about foreign pensions, including the pension amount, periods of employment or self-employment the pension is based on, and if these are tied to Social Security through Totalization Agreements between the U.S. and other countries. This information influences the determination of U.S. Social Security retirement or disability benefits, ensuring a fair assessment where benefits are recalculated to reflect genuine lifetime earnings. Significantly, WEP aims to adjust benefits for individuals who have not contributed to the Social Security system throughout their careers, considering their non-covered foreign work. Completing the SSA-308 accurately is thus fundamental for individuals in this situation, as errors or omissions could affect their benefits. Additionally, the form binds the individual to notify the Social Security Administration (SSA) of any changes in their pension status, reinforcing the importance of accurate, up-to-date information for benefit calculation. Acknowledging the sensitivity of the data collected, the form also outlines privacy guidelines and the legal implications of providing false information, emphasizing the seriousness of the process and the commitment to maintaining individuals' privacy.
| Question | Answer |
|---|---|
| Form Name | Form Ssa 308 |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | ssa 308 pdf, pension social security form, pension social security administration form, pension social form |