

supplemental security income can be filled in online without any problem. Simply make use of FormsPal PDF tool to get it done without delay. The editor is continually upgraded by our staff, receiving powerful functions and becoming better. To get the process started, consider these easy steps:
Step 1: Click the "Get Form" button in the top section of this webpage to access our tool.
Step 2: This tool provides you with the capability to work with almost all PDF documents in many different ways. Enhance it with your own text, correct existing content, and add a signature - all possible within minutes!
This PDF doc will require you to type in specific information; to ensure consistency, please be sure to consider the following suggestions:
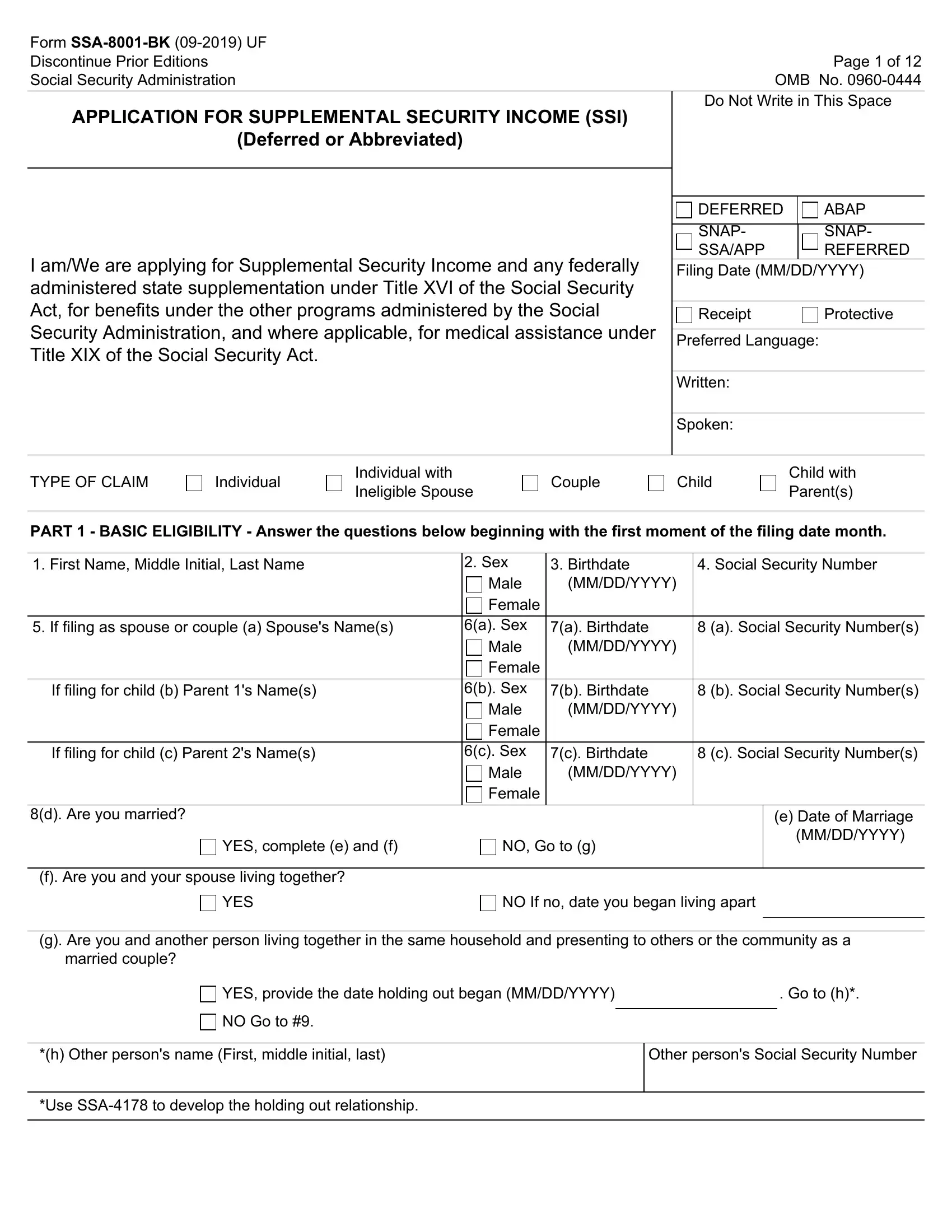
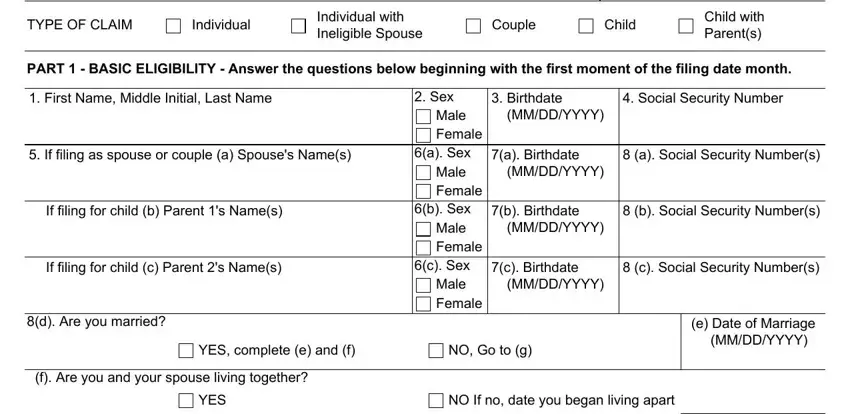
1. Begin completing the supplemental security income with a number of necessary fields. Get all the information you need and be sure there is nothing forgotten!
2. Now that the last part is completed, you should put in the needed specifics in married couple, YES provide the date holding out, NO Go to, h Other persons name First middle, Other persons Social Security, and Use SSA to develop the holding out so you can proceed to the next stage.
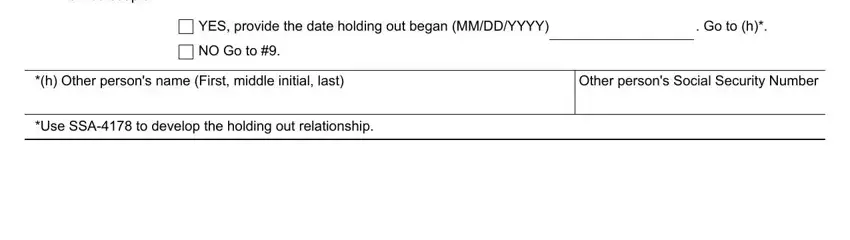
Many people generally get some things incorrect when completing Use SSA to develop the holding out in this part. You should reread whatever you enter right here.
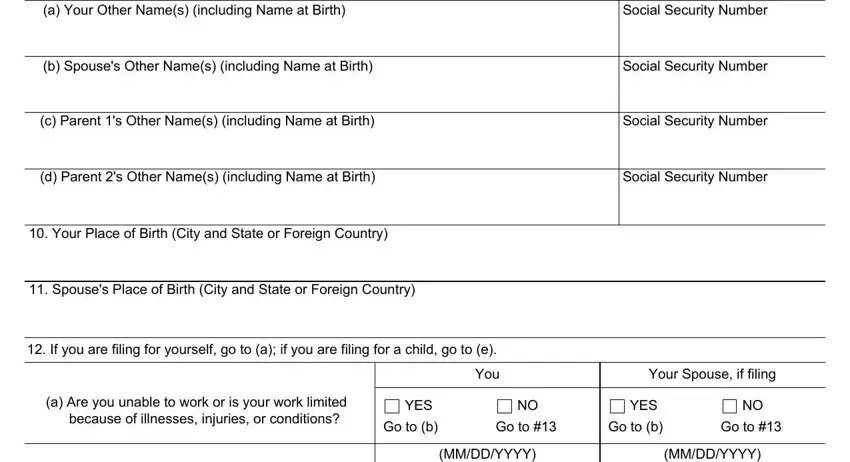
3. Completing a Your Other Names including Name, Social Security Number, b Spouses Other Names including, Social Security Number, c Parent s Other Names including, Social Security Number, d Parent s Other Names including, Social Security Number, Your Place of Birth City and, Spouses Place of Birth City and, If you are filing for yourself go, a Are you unable to work or is, because of illnesses injuries or, YES, and Go to b is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
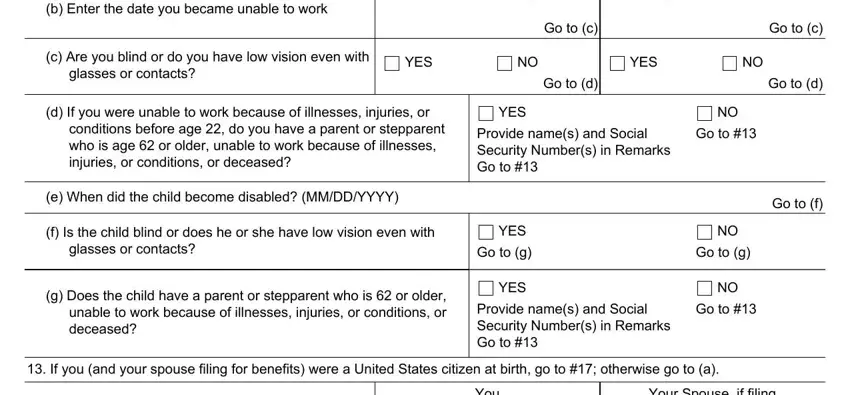
4. To go forward, the next step requires filling out a few fields. Included in these are b Enter the date you became unable, MMDDYYYY, MMDDYYYY, Go to c, c Are you blind or do you have low, glasses or contacts, YES, YES, Go to d, d If you were unable to work, YES, conditions before age do you have, Provide names and Social Security, Go to, and e When did the child become, which are key to moving forward with this document.
5. As a final point, this final part is precisely what you need to complete prior to submitting the PDF. The blanks here are the next: You, Your Spouse if filing, a Are you a naturalized United, YES, YES, Go to, Go to b, Go to, Go to b, b Are you an American Indian born, United States, YES, Go to c, Go to d, and YES.
Step 3: Before addressing the next step, it's a good idea to ensure that all form fields were filled out the right way. When you think it's all fine, click “Done." Grab the supplemental security income when you register here for a free trial. Quickly view the pdf form in your FormsPal cabinet, with any modifications and adjustments conveniently synced! FormsPal provides secure form editing without personal information record-keeping or any sort of sharing. Rest assured that your details are secure with us!