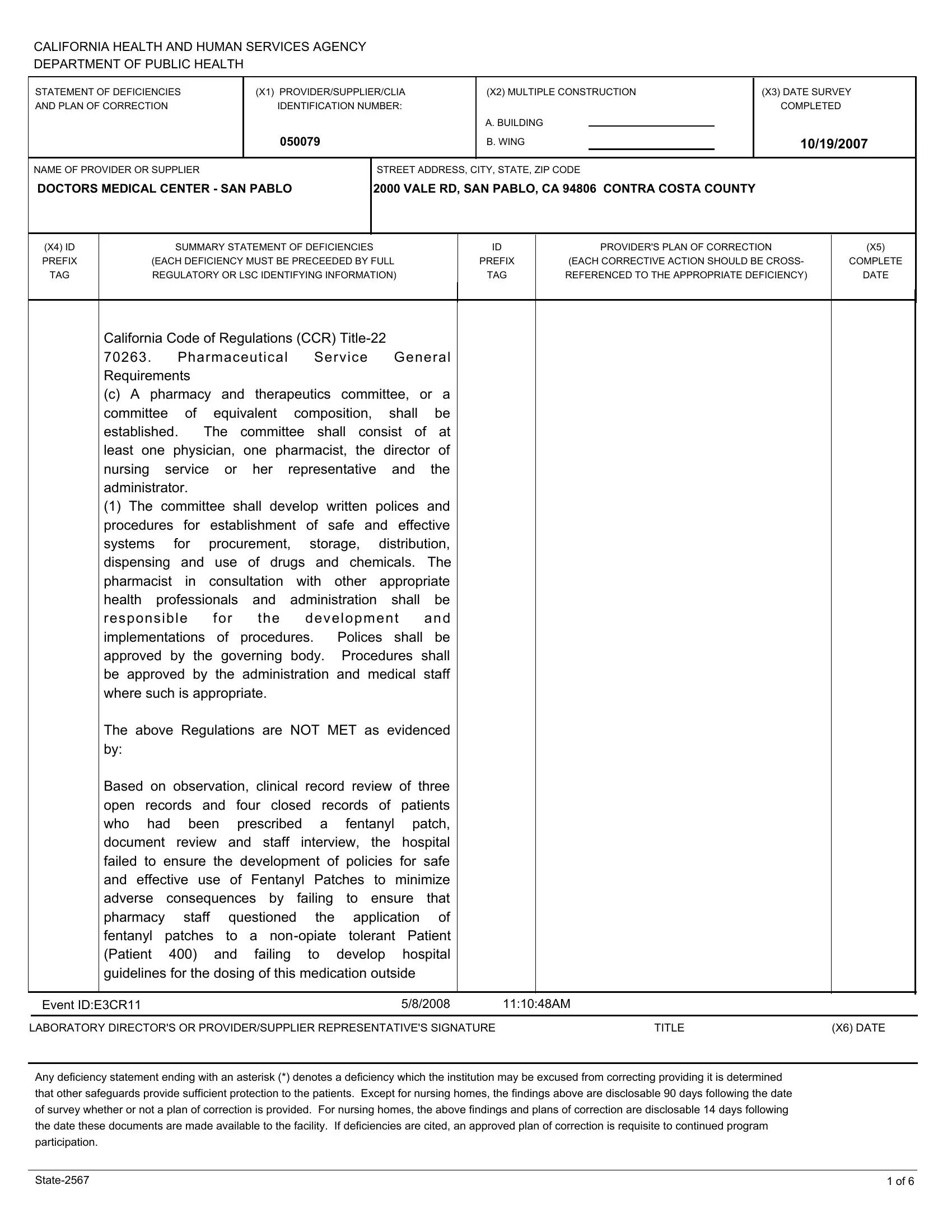
The State 2567 form is a critical document used by the California Health and Human Services Agency, Department of Public Health, to outline deficiencies found in healthcare providers or suppliers during surveys. As observed in the October 2007 survey of Doctors Medical Center - San Pablo, located in Contra Costa County, the form meticulously details the areas where the facility did not meet specific regulatory requirements, such as the management and safe use of pharmaceuticals, notably Fentanyl Patches. These details include the lack of development of policies for the safe and effective use of such medications and the absence of pharmacy staff’s intervention in verifying the opioid tolerance of patients before prescribing potent opioid medications. Furthermore, the form highlights the provider’s plan of correction for each deficiency cited, underlining the importance of compliance and corrective actions in maintaining high standards of patient care and safety. The form also outlines regulations regarding the disclosure of findings and the necessity of an approved plan of correction for continued program participation, emphasizing accountability and the prioritization of patient safety in healthcare settings. In essence, the State 2567 form serves as a vital tool for healthcare quality assurance, ensuring that facilities adhere to established guidelines and regulations to mitigate risks and improve patient care outcomes.
| Question | Answer |
|---|---|
| Form Name | Form State 2567 |
| Form Length | 6 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min 30 sec |
| Other names | 2567DoctorsMedi calCenter SanPablo Event E3CR11 california code of regulations title 22 70263 form |