
Form Vb01 can be completed with ease. Simply make use of FormsPal PDF tool to get it done in a timely fashion. Our editor is continually evolving to give the best user experience possible, and that's because of our resolve for continual enhancement and listening closely to testimonials. With some basic steps, you can begin your PDF journey:
Step 1: Click on the "Get Form" button above on this page to open our editor.
Step 2: This tool gives you the capability to modify your PDF document in many different ways. Modify it by writing personalized text, adjust existing content, and include a signature - all within several mouse clicks!
This PDF doc requires specific information; to guarantee consistency, don't hesitate to consider the following tips:
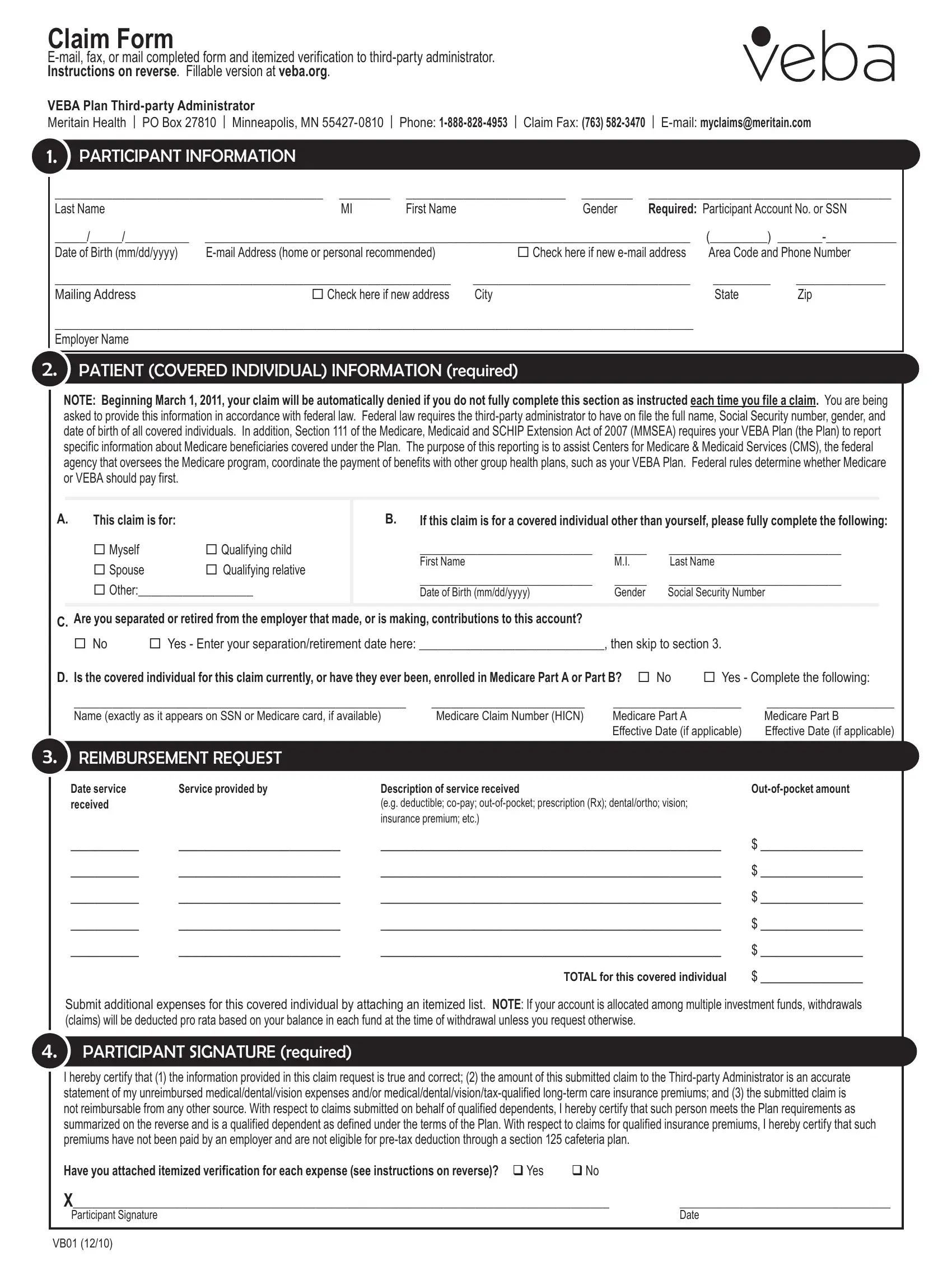
1. Whenever completing the Form Vb01, be certain to include all needed blanks in its associated section. This will help to hasten the work, allowing your information to be handled efficiently and appropriately.
2. The subsequent stage would be to fill out the next few fields: Are you separated or retired from, No Yes Enter your, Is the covered individual for this, Name exactly as it appears on, reimBursement reQuest, Date service received, Service provided by, Description of service received eg, TOTAL for this covered individual, Outofpocket amount, Submit additional expenses for, participant signature required, and I hereby certify that the.
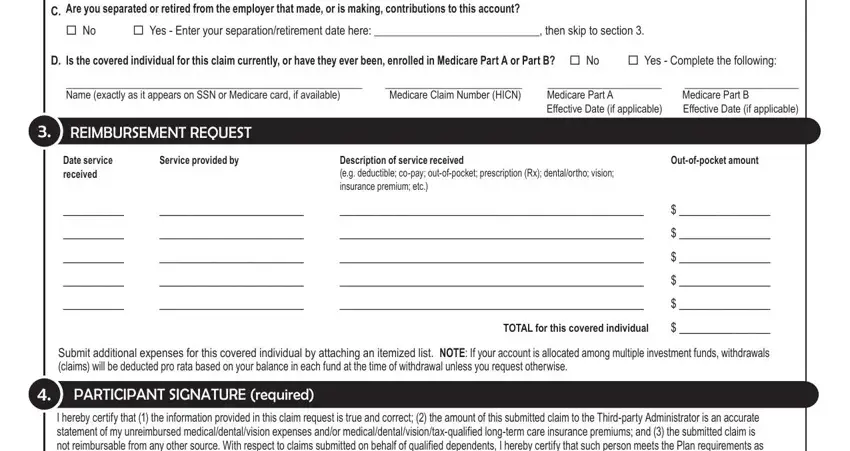
Always be extremely mindful while completing Service provided by and No Yes Enter your, since this is where a lot of people make a few mistakes.
3. In this particular step, look at I hereby certify that the, Have you attached itemized, X Participant Signature, and Date. These need to be filled in with utmost accuracy.

Step 3: You should make sure your information is correct and simply click "Done" to proceed further. Create a 7-day free trial option at FormsPal and obtain instant access to Form Vb01 - accessible from your FormsPal account. FormsPal guarantees your data privacy by using a protected system that in no way saves or distributes any sort of personal data involved. Feel safe knowing your documents are kept confidential whenever you use our editor!