
By using the online tool for PDF editing by FormsPal, you are able to complete or modify Form Vcgcb Vcp 005 here and now. FormsPal team is aimed at providing you the ideal experience with our editor by consistently presenting new capabilities and upgrades. Our editor has become a lot more user-friendly as the result of the newest updates! Currently, editing documents is a lot easier and faster than ever. Getting underway is simple! All you have to do is take the next easy steps below:
Step 1: Hit the "Get Form" button above. It's going to open our editor so you could begin filling in your form.
Step 2: As you access the online editor, there'll be the document ready to be filled out. Besides filling in various blank fields, it's also possible to perform some other actions with the form, specifically putting on custom text, changing the initial text, adding images, placing your signature to the document, and a lot more.
In order to fill out this PDF form, make sure that you enter the information you need in every blank field:
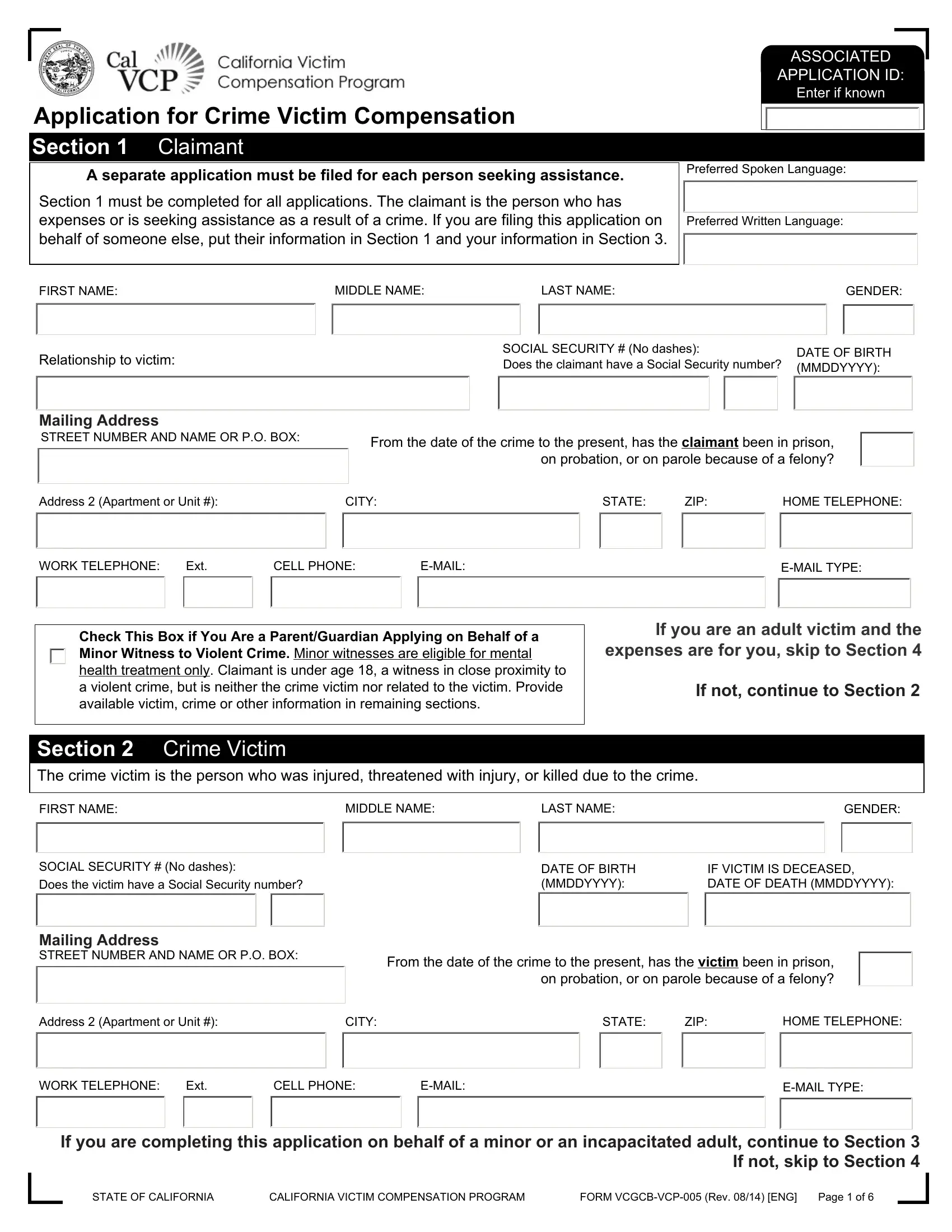
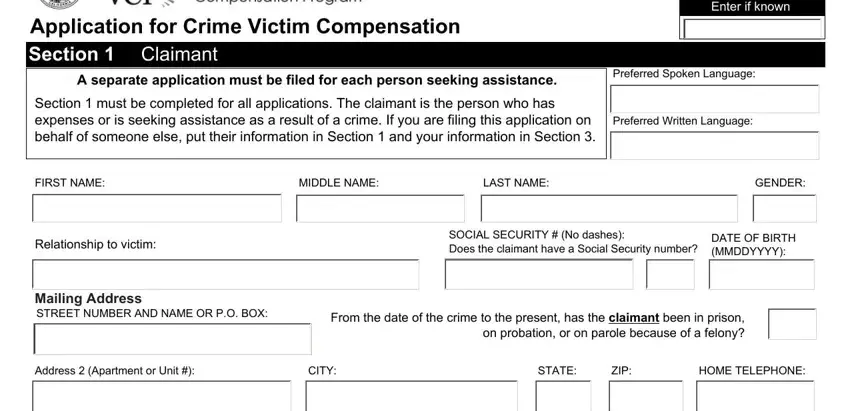
1. Begin filling out your Form Vcgcb Vcp 005 with a selection of essential fields. Get all of the information you need and make certain nothing is omitted!
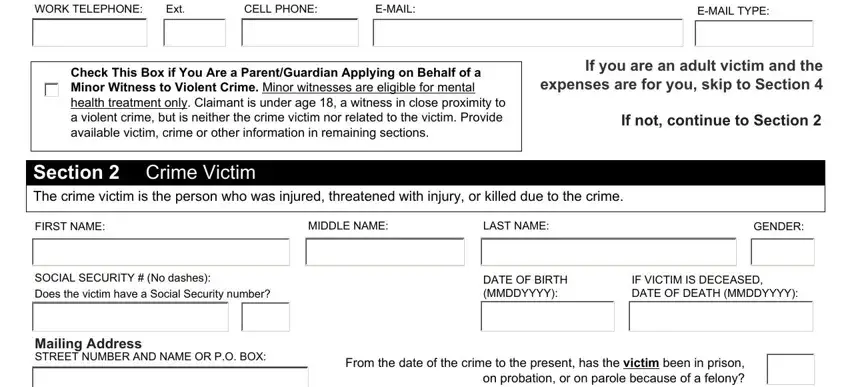
2. Once your current task is complete, take the next step – fill out all of these fields - WORK TELEPHONE, Ext, CELL PHONE, EMAIL, EMAIL TYPE, Check This Box if You Are a, If you are an adult victim and the, If not continue to Section, Section The crime victim is the, Crime Victim, FIRST NAME, MIDDLE NAME, LAST NAME, GENDER, and SOCIAL SECURITY No dashes Does with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
3. In this specific step, look at Address Apartment or Unit, CITY, STATE, ZIP, HOME TELEPHONE, WORK TELEPHONE, Ext, CELL PHONE, EMAIL, EMAIL TYPE, If you are completing this, STATE OF CALIFORNIA, CALIFORNIA VICTIM COMPENSATION, FORM VCGCBVCP Rev ENG, and Page of. All these will have to be taken care of with utmost accuracy.
It is easy to make a mistake while filling out your If you are completing this, consequently make sure to go through it again prior to when you finalize the form.
4. The subsequent part requires your details in the subsequent parts: This section is for parents or, FIRST NAME, MIDDLE NAME, LAST NAME, GENDER, SOCIAL SECURITY No dashes Does, DATE OF BIRTH MMDDYYYY, Mailing Address STREET NUMBER AND, From the date of the crime to the, Address Apartment or Suite, CITY, STATE, ZIP, HOME TELEPHONE, and WORK TELEPHONE. Always fill out all requested info to go further.
5. Last of all, this last segment is precisely what you'll have to finish prior to using the PDF. The blanks under consideration include the following: Medical andor dental expenses, Moving or relocation expenses, Job retraining for a victim, Other crimerelated expenses, Mental health treatment, Home security improvements, Crime scene cleanup, Income loss if you missed work, Home or vehicle modifications for, For someone other than the victim, For minor witnesses to violent, Mental health treatment, Funeral andor burial expenses, Medical expenses for a deceased, and Wage loss up to days if a minor.
Step 3: Reread everything you have entered into the form fields and then click the "Done" button. Download your Form Vcgcb Vcp 005 as soon as you register here for a 7-day free trial. Easily gain access to the document within your FormsPal cabinet, along with any edits and adjustments being automatically saved! FormsPal guarantees your information privacy by using a secure system that never records or shares any type of personal data used in the form. Feel safe knowing your docs are kept confidential each time you use our tools!