

Handling PDF forms online is always simple with our PDF editor. You can fill in ct form w 1qmb here within minutes. In order to make our editor better and simpler to work with, we continuously implement new features, with our users' feedback in mind. With just a few simple steps, you are able to begin your PDF editing:
Step 1: Access the PDF in our editor by hitting the "Get Form Button" in the top section of this webpage.
Step 2: This editor grants the ability to change most PDF files in a variety of ways. Enhance it by writing your own text, correct existing content, and put in a signature - all close at hand!
In order to fill out this document, ensure that you enter the information you need in every blank:
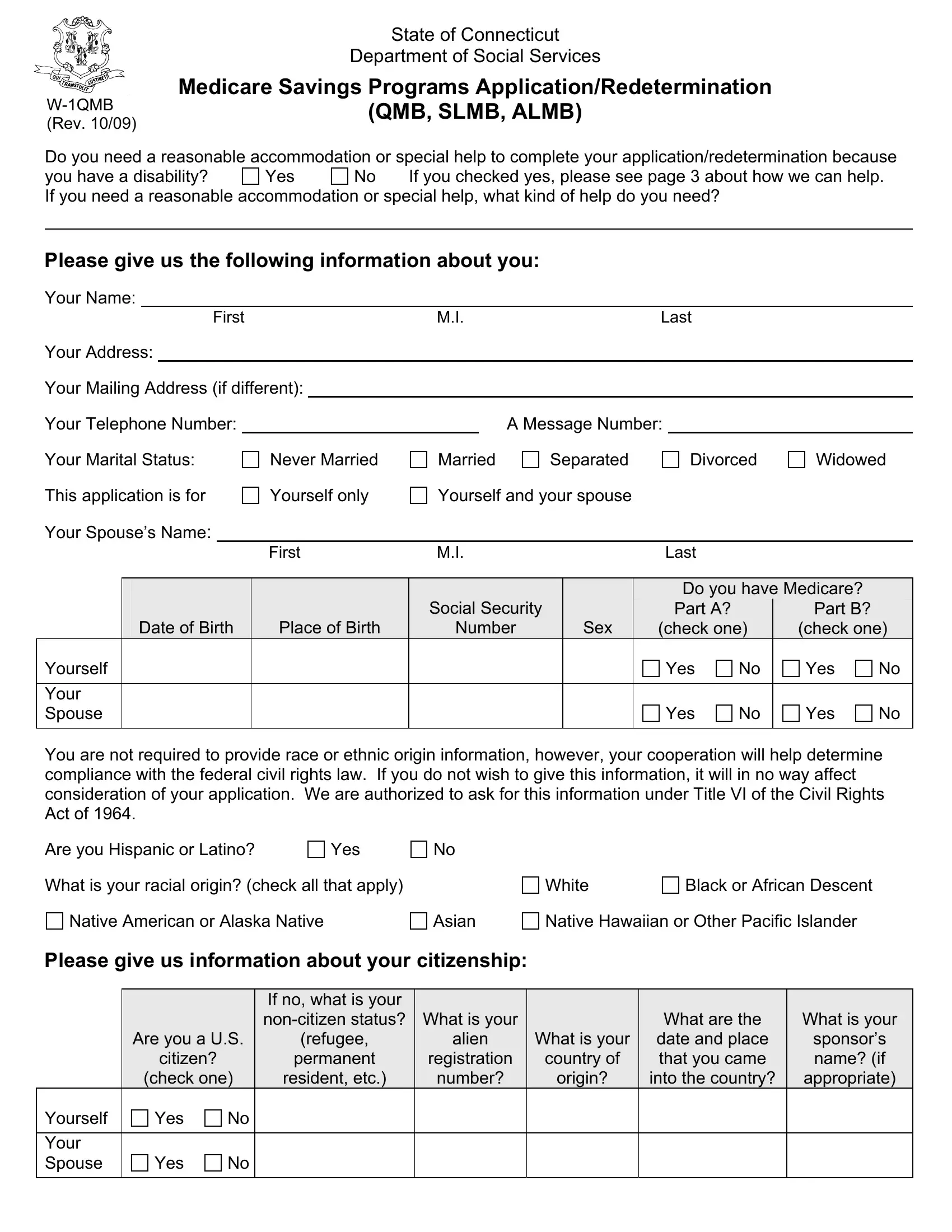
1. You will need to complete the ct form w 1qmb correctly, therefore take care while working with the parts including all of these fields:
2. Just after finishing the previous part, go to the next part and fill out the essential particulars in these fields - Date of Birth, Place of Birth, Number, Sex, check one, check one, Yourself Your Spouse You are not, Yes, Yes, Yes, Yes, Are you Hispanic or Latino, Yes, What is your racial origin check, and White.
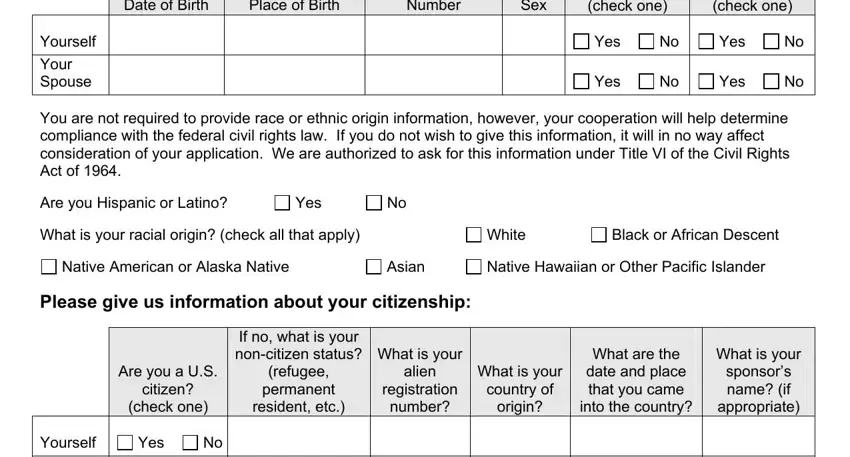
In terms of Sex and Date of Birth, make certain you do everything right here. The two of these are viewed as the most important ones in this page.
3. This next segment is mostly about Yourself Your Spouse, and Yes - type in each of these empty form fields.

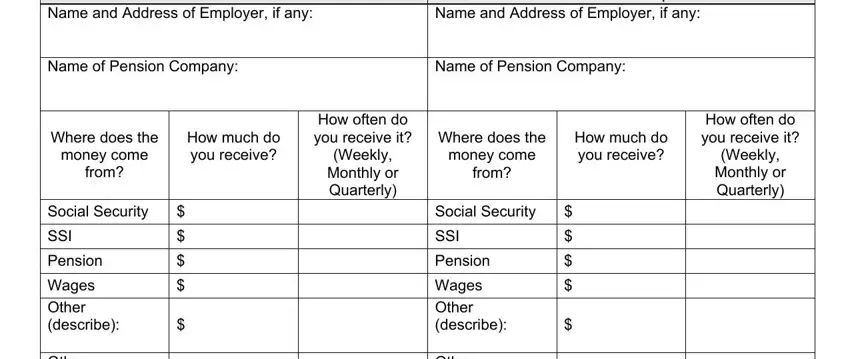
4. This next section requires some additional information. Ensure you complete all the necessary fields - Income for Yourself, Name and Address of Employer if, Income for Your Spouse Name and, Where does the, money come, How much do you receive, from, Social Security, SSI, Pension, Wages Other describe Other describe, How often do you receive it, Weekly Monthly or Quarterly, Where does the, and money come - to proceed further in your process!
5. This final notch to finalize this document is crucial. Make sure that you fill out the necessary form fields, such as Wages Other describe Other describe, Other describe, I authorize the Department of, Signature of Spouse, Date, and Date, before finalizing. If not, it could end up in a flawed and possibly unacceptable paper!
Step 3: Proofread the details you have typed into the blank fields and click the "Done" button. Sign up with us right now and instantly use ct form w 1qmb, available for downloading. All changes you make are preserved , meaning you can edit the pdf at a later point anytime. When using FormsPal, you can certainly fill out forms without being concerned about information incidents or records getting shared. Our protected platform ensures that your personal data is maintained safe.