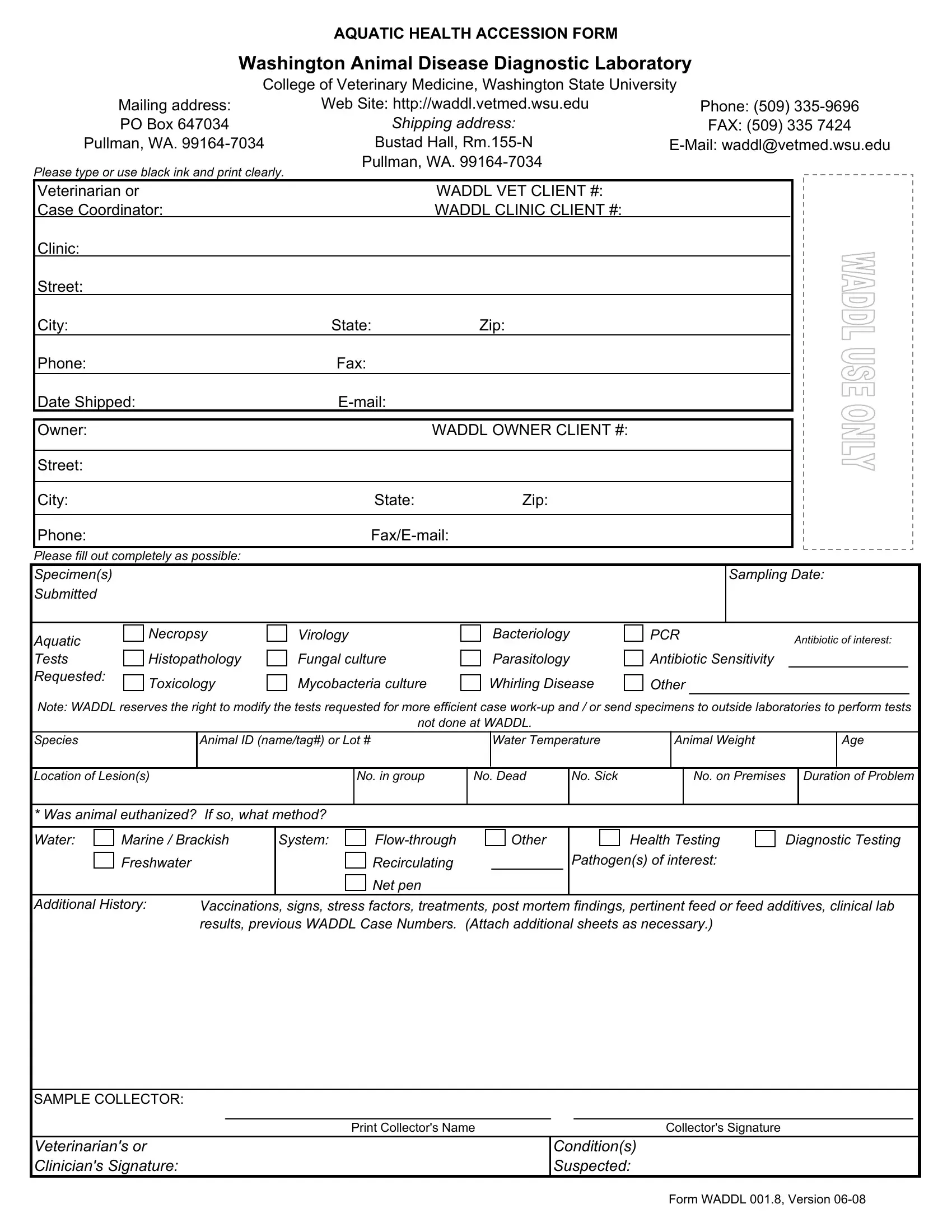
The Waddl 001 8 form, known as the Aquatic Health Accession Form, plays a crucial role in diagnosing and managing diseases within aquatic animal populations. Created by the Washington Animal Disease Diagnostic Laboratory at the College of Veterinary Medicine, Washington State University, this comprehensive document serves as a pivotal tool for veterinarians, researchers, and aquatic animal owners. It facilitates the submission of samples for a variety of tests, including but not limited to virology, bacteriology, parasitology, and toxicology. Detailed instructions stress the importance of using black ink and printing clearly to ensure accurate information recording. Its layout prompts for exhaustive details about the specimen, ranging from the species and water temperature to the health and environmental conditions surrounding the aquatic animal. The form also emphasizes the collaborative effort between the submitter and the diagnostic laboratory by requesting extensive background information, such as history of vaccinations, signs of illness, and previous diagnostic findings. The flexibility of the form is evident in its provision for WADDL to adjust tests or refer them to external laboratories, ensuring a tailored and efficient diagnostic approach. This document underscores the laboratory's commitment to fostering aquatic animal health through precise diagnostic practices.
| Question | Answer |
|---|---|
| Form Name | Form Waddl 001 8 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | Accession AquaticHealthWA DDL 001.8 waddl aquatic health accession form |
AQUATIC HEALTH ACCESSION FORM
Washington Animal Disease Diagnostic Laboratory
|
College of Veterinary Medicine, Washington State University |
|
|||
|
Mailing address: |
Web Site: http://waddl.vetmed.wsu.edu |
|
Phone: (509) |
|
|
PO Box 647034 |
Shipping address: |
|
FAX: (509) 335 7424 |
|
Pullman, WA. |
Bustad Hall, |
||||
Please type or use black ink and print clearly. |
Pullman, WA. |
|
|
||
|
|
|
|
||
Veterinarian or |
|
WADDL VET CLIENT #: |
|
|
|
Case Coordinator: |
|
WADDL CLINIC CLIENT #: |
|
|
|
Clinic: |
|
|
|
|
|
Street: |
|
|
|
|
|
City: |
|
State: |
Zip: |
|
|
Phone: |
|
Fax: |
|
|
|
Date Shipped: |
|
|
|
||
Owner: |
|
|
WADDL OWNER CLIENT #: |
|
|
Street: |
|
|
|
|
|
City: |
|
State: |
Zip: |
|
|
Phone: |
|
|
|
||
Please fill out completely as possible: |
|
|
|
|
|
Specimen(s) |
|
|
|
|
Sampling Date: |
Submitted |
|
|
|
|
|
Aquatic |
Necropsy |
Virology |
Bacteriology |
PCR |
Antibiotic of interest: |
|
|
|
|
||
Tests |
Histopathology |
Fungal culture |
Parasitology |
Antibiotic Sensitivity |
|
Requested: |
Toxicology |
Mycobacteria culture |
Whirling Disease |
Other |
|
|
|
||||
Note: WADDL reserves the right to modify the tests requested for more efficient case
not done at WADDL.
Species |
|
|
Animal ID (name/tag#) or Lot # |
|
|
Water Temperature |
|
Animal Weight |
|
|
Age |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Location of Lesion(s) |
|
|
|
|
No. in group |
No. Dead |
|
|
No. Sick |
|
|
No. on Premises |
Duration of Problem |
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
* Was animal euthanized? If so, what method? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Water: |
|
Marine / Brackish |
System: |
|
|
|
|
|
Other |
|
|
|
|
|
Health Testing |
|
|
Diagnostic Testing |
|||||||||
|
|
Freshwater |
|
|
|
|
|
Recirculating |
|
|
|
|
|
|
Pathogen(s) of interest: |
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
Net pen |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Additional History: |
Vaccinations, signs, stress factors, treatments, post mortem findings, pertinent feed or feed additives, clinical lab |
||||||||||||||||||||||||||
|
|
|
results, previous WADDL Case Numbers. (Attach additional sheets as necessary.) |
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SAMPLE COLLECTOR: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
Print Collector's Name |
|
|
|
|
|
|
Collector's Signature |
|
|
|
|
||||||||||
Veterinarian's or |
|
|
|
|
|
|
|
|
|
|
Condition(s) |
|
|
|
|
|
|
|
|
|
|||||||
Clinician's Signature: |
|
|
|
|
|
|
|
|
|
|
Suspected: |
|
|
|
|
|
|
|
|
|
|||||||
Form WADDL 001.8, Version