
Dealing with PDF documents online can be quite easy with our PDF editor. Anyone can fill out CALIFORNIA here painlessly. To keep our tool on the leading edge of practicality, we work to put into operation user-driven features and enhancements on a regular basis. We're routinely thankful for any suggestions - help us with reshaping how you work with PDF forms. With a few basic steps, you are able to start your PDF editing:
Step 1: Access the PDF file inside our tool by clicking on the "Get Form Button" at the top of this page.
Step 2: The editor provides you with the capability to work with the majority of PDF forms in a variety of ways. Transform it by including customized text, correct what is already in the PDF, and include a signature - all when you need it!
It will be simple to complete the pdf with our detailed tutorial! This is what you have to do:
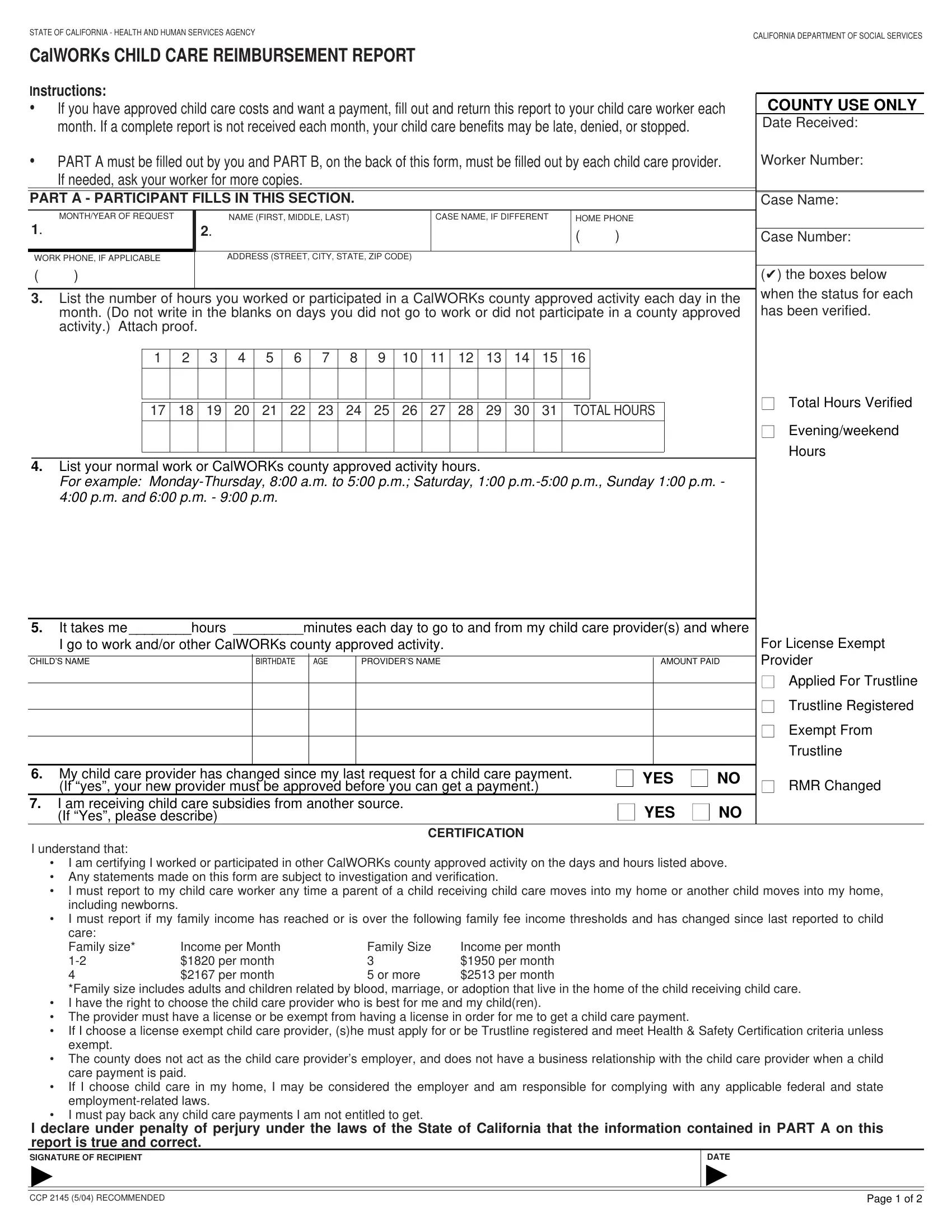
1. For starters, once filling in the CALIFORNIA, beging with the form section that features the subsequent blanks:
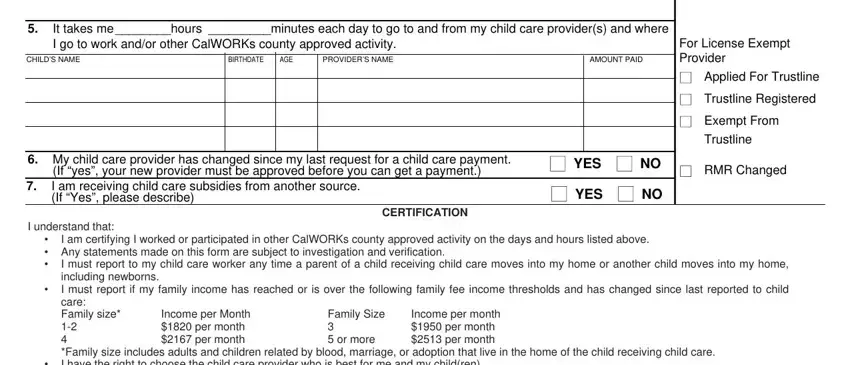
2. After completing the last step, head on to the subsequent part and complete the necessary details in all these blanks - It takes me hours minutes each day, AMOUNT PAID, BIRTHDATE, AGE, CHILDS NAME, My child care provider has, If yes your new provider must be, I understand that, CERTIFICATION, YES YES, For License Exempt Provider, Applied For Trustline, Trustline Registered, Exempt From Trustline, and RMR Changed.
3. The following segment is all about I declare under penalty of perjury, DATE, CCP RECOMMENDED, and Page of - fill in each of these blank fields.

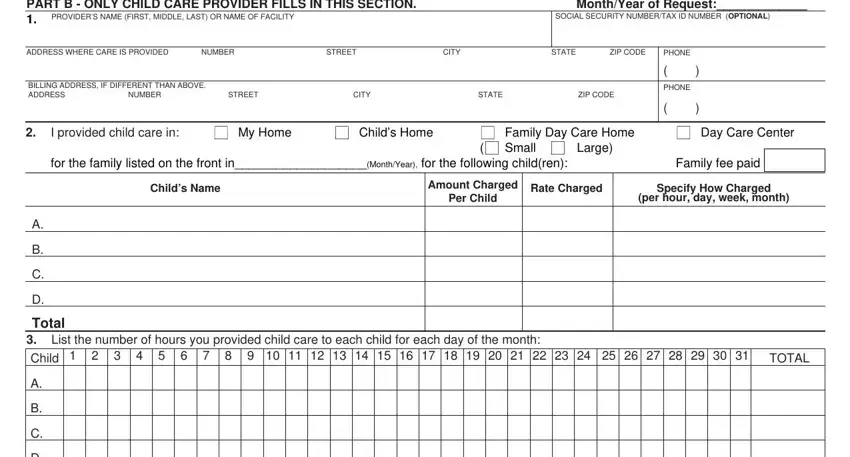
4. Filling in PART B ONLY CHILD CARE PROVIDER, PROVIDERS NAME FIRST MIDDLE LAST, SOCIAL SECURITY NUMBERTAX ID, ADDRESS WHERE CARE IS PROVIDED, NUMBER, STREET, CITY, STATE, ZIP CODE, PHONE, BILLING ADDRESS IF DIFFERENT THAN, NUMBER, STREET, CITY, and STATE is vital in this form section - you'll want to don't hurry and take a close look at each and every empty field!
You can certainly make a mistake when filling in your CITY, so be sure you go through it again before you send it in.
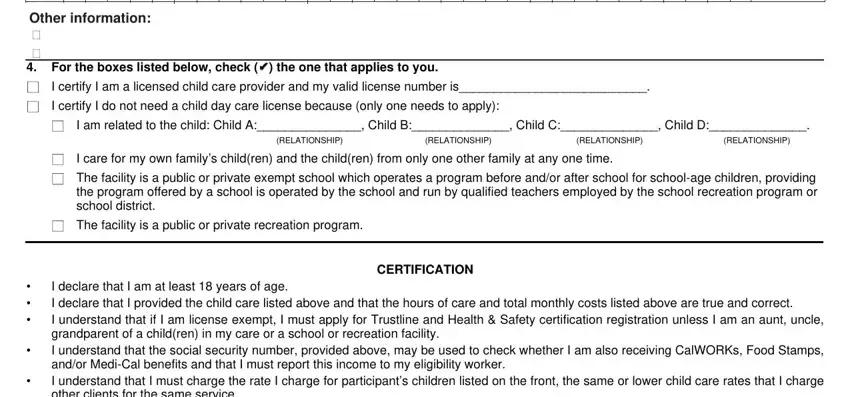
5. The very last step to finish this form is essential. Be sure you fill in the appropriate form fields, and this includes Other information cid, cid For the boxes listed below, the one that applies to you, I certify I am a licensed child, I certify I do not need a child, I am related to the child Child A, RELATIONSHIP, RELATIONSHIP, RELATIONSHIP, RELATIONSHIP, I care for my own familys children, The facility is a public or, The facility is a public or, CERTIFICATION, and cid cid cid, before using the form. Or else, it might lead to a flawed and potentially incorrect paper!
Step 3: When you have looked over the information in the blanks, click "Done" to finalize your document creation. Right after starting a7-day free trial account at FormsPal, you will be able to download CALIFORNIA or email it immediately. The form will also be readily available from your personal account with your each modification. FormsPal is invested in the privacy of our users; we ensure that all information put into our tool remains protected.