

With the help of the online PDF editor by FormsPal, it is possible to fill in or alter ut ability form right here. To have our tool on the leading edge of practicality, we strive to integrate user-oriented features and improvements on a regular basis. We're routinely looking for feedback - join us in reshaping how you work with PDF documents. To get the process started, consider these simple steps:
Step 1: Just press the "Get Form Button" at the top of this webpage to start up our pdf editing tool. This way, you will find all that is required to fill out your document.
Step 2: Using this handy PDF editing tool, you can do more than merely fill out blank form fields. Edit away and make your forms appear perfect with customized textual content incorporated, or fine-tune the original content to excellence - all that backed up by the capability to add any kind of graphics and sign the file off.
Completing this PDF generally requires focus on details. Make certain every field is completed accurately.
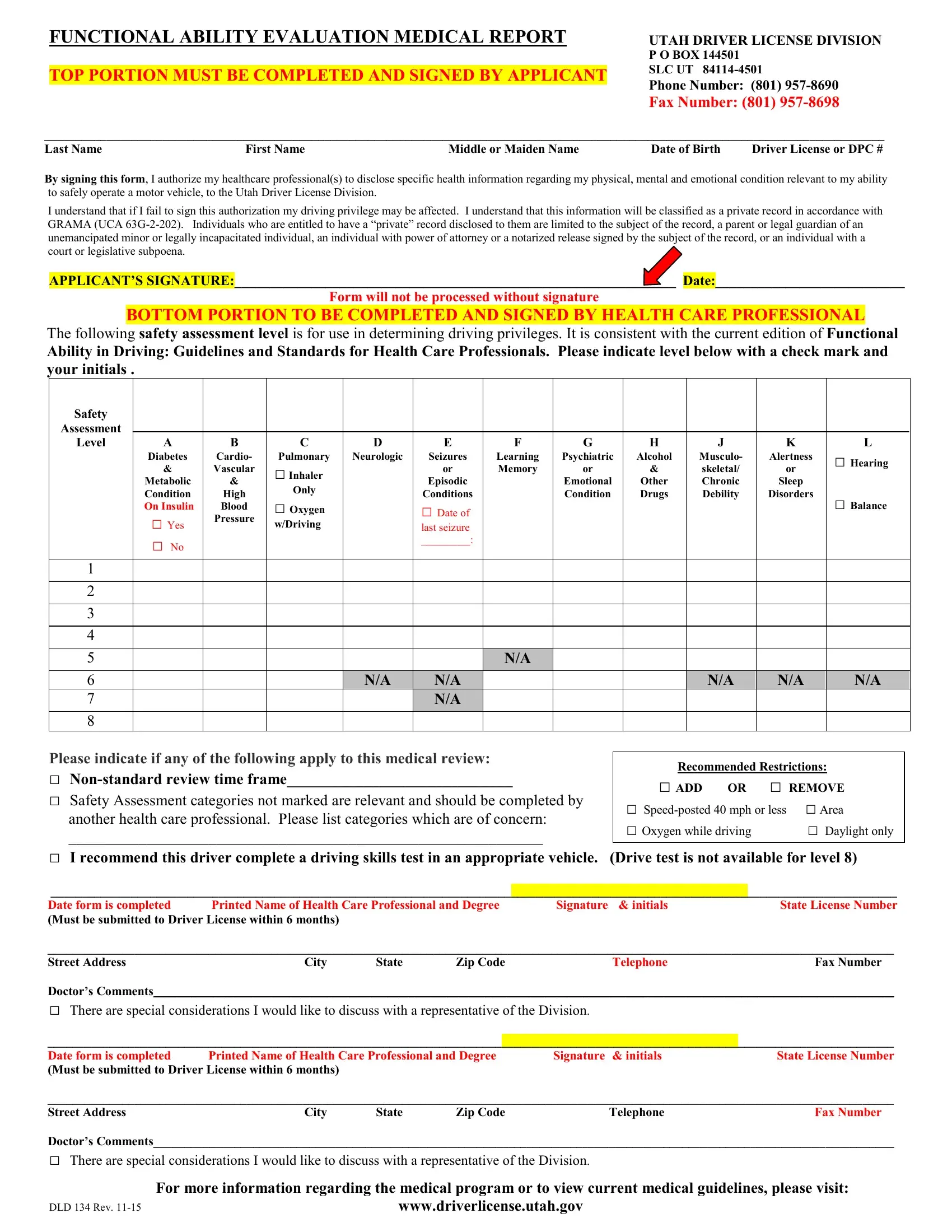
1. To start off, once filling in the ut ability form, begin with the section that features the next fields:
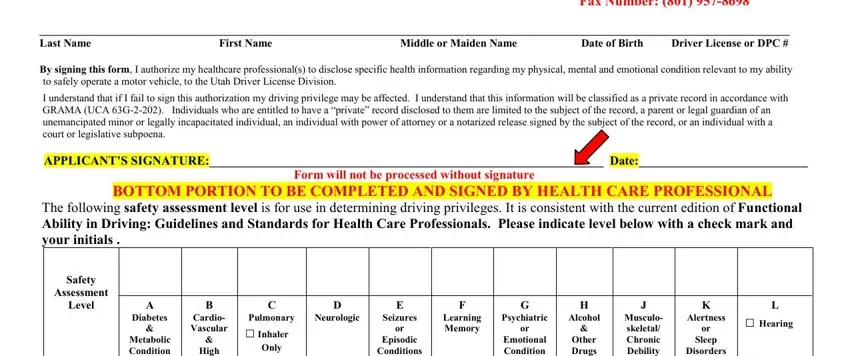
2. Soon after this section is completed, go to enter the suitable information in these: Emotional Condition, Other Drugs, Musculo skeletal Chronic Debility, Disorders, Hearing Balance, High Blood, Pressure, Metabolic Condition On Insulin, Yes No, Inhaler Oxygen, wDriving, Conditions, Date of, last seizure, and NA NA.
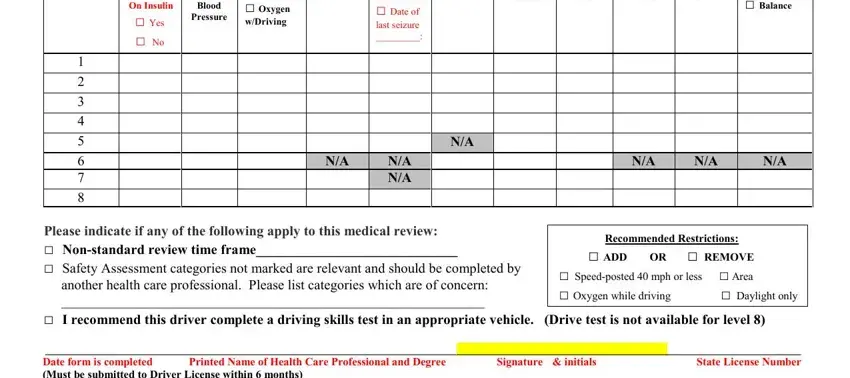
Always be really careful when filling in Pressure and Emotional Condition, as this is the part where a lot of people make some mistakes.
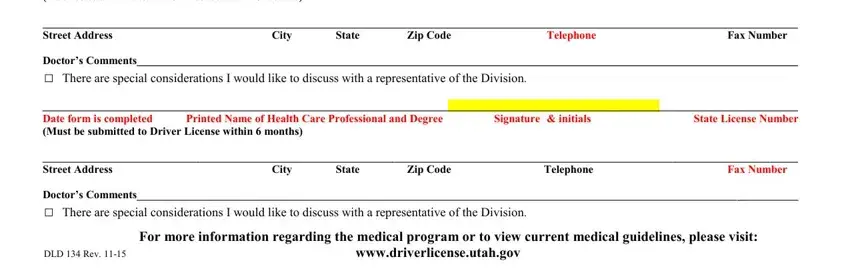
3. This 3rd step is considered fairly simple, Date form is completed Printed, City State Zip Code, Fax Number, Telephone, Doctors Comments, There are special considerations, Date form is completed Printed, Telephone Fax Number, City State Zip Code, There are special considerations, and DLD Rev wwwdriverlicenseutahgov - every one of these empty fields needs to be completed here.
Step 3: Prior to moving forward, make sure that all form fields were filled out correctly. The moment you’re satisfied with it, click “Done." Make a free trial option with us and get instant access to ut ability form - downloadable, emailable, and editable from your personal cabinet. If you use FormsPal, you're able to complete forms without needing to be concerned about database leaks or records being distributed. Our secure platform helps to ensure that your personal information is stored safely.