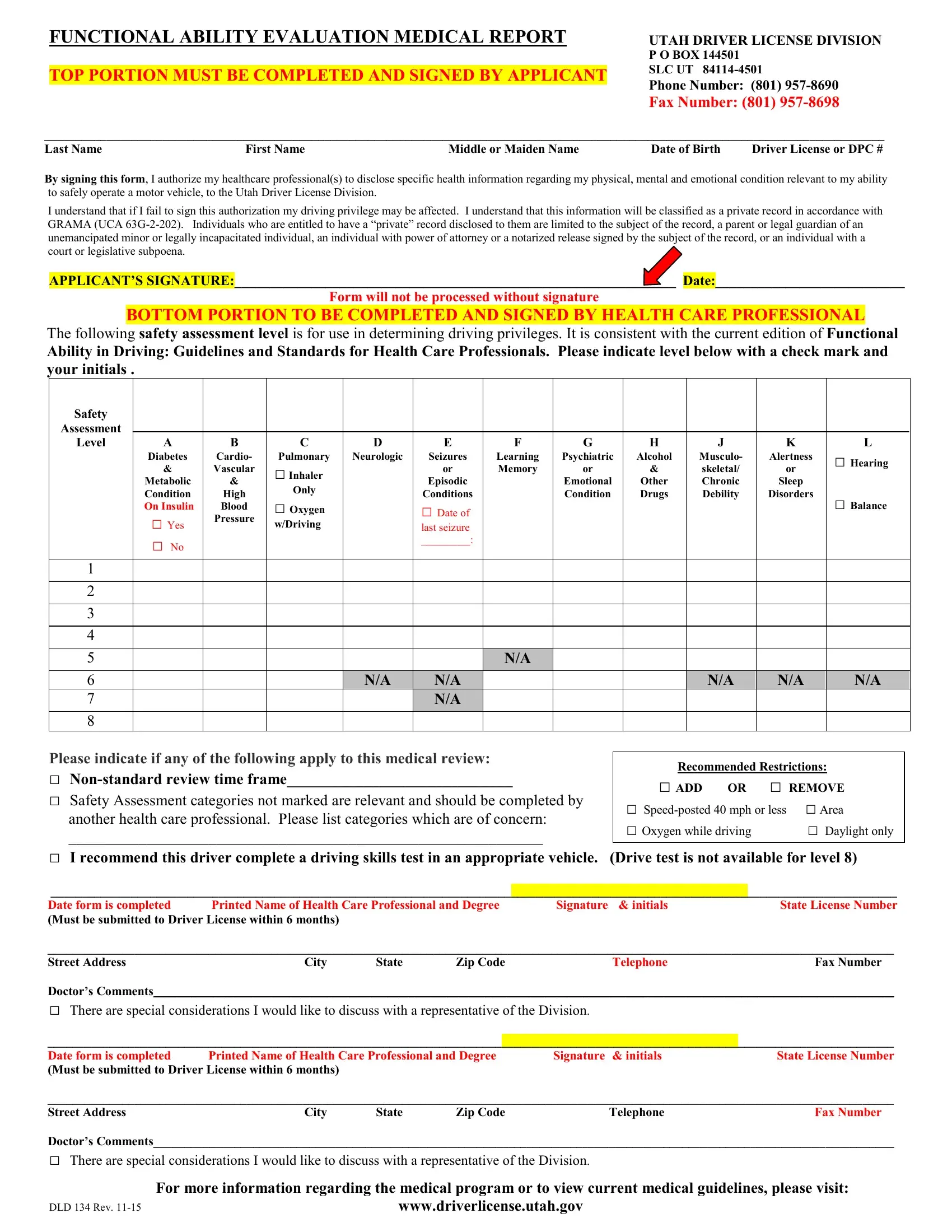
The Functional Ability Medical Report form occupies a crucial position in evaluating an individual's ability to safely operate a motor vehicle, particularly in Utah. This form bridges the communication between healthcare professionals and the Utah Driver License Division, ensuring that individuals with medical conditions that might affect their driving capability are appropriately assessed. The applicant's consent is foundational, as it permits healthcare providers to share relevant health information. This consent is critical not only for the protection of the individual's privacy rights but also for the broader public safety concern. Each section of the form, from the applicant's personal information to the detailed health assessment conducted by a healthcare professional, is designed to capture essential data. The healthcare professional evaluates the applicant's physical, mental, and emotional fitness against a standardized safety assessment. This assessment meticulously categorizes the impact of various conditions, such as neurological disorders, diabetes, and cardiovascular issues, on driving abilities. Recommendations for restrictions or the need for a driving skills test further tailor the approach to each applicant's unique circumstances. The form also provides space for professionals to note any exceptional considerations, ensuring a comprehensive review process. This careful balance between individual rights and public safety underscores the form's importance, providing a structured pathway for making informed decisions about driving privileges.
| Question | Answer |
|---|---|
| Form Name | Functional Ability Medical Report Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | ut ability form, utah functional ability evaluation medical report, dmv functional ability form utah, utah drivers license medical form |