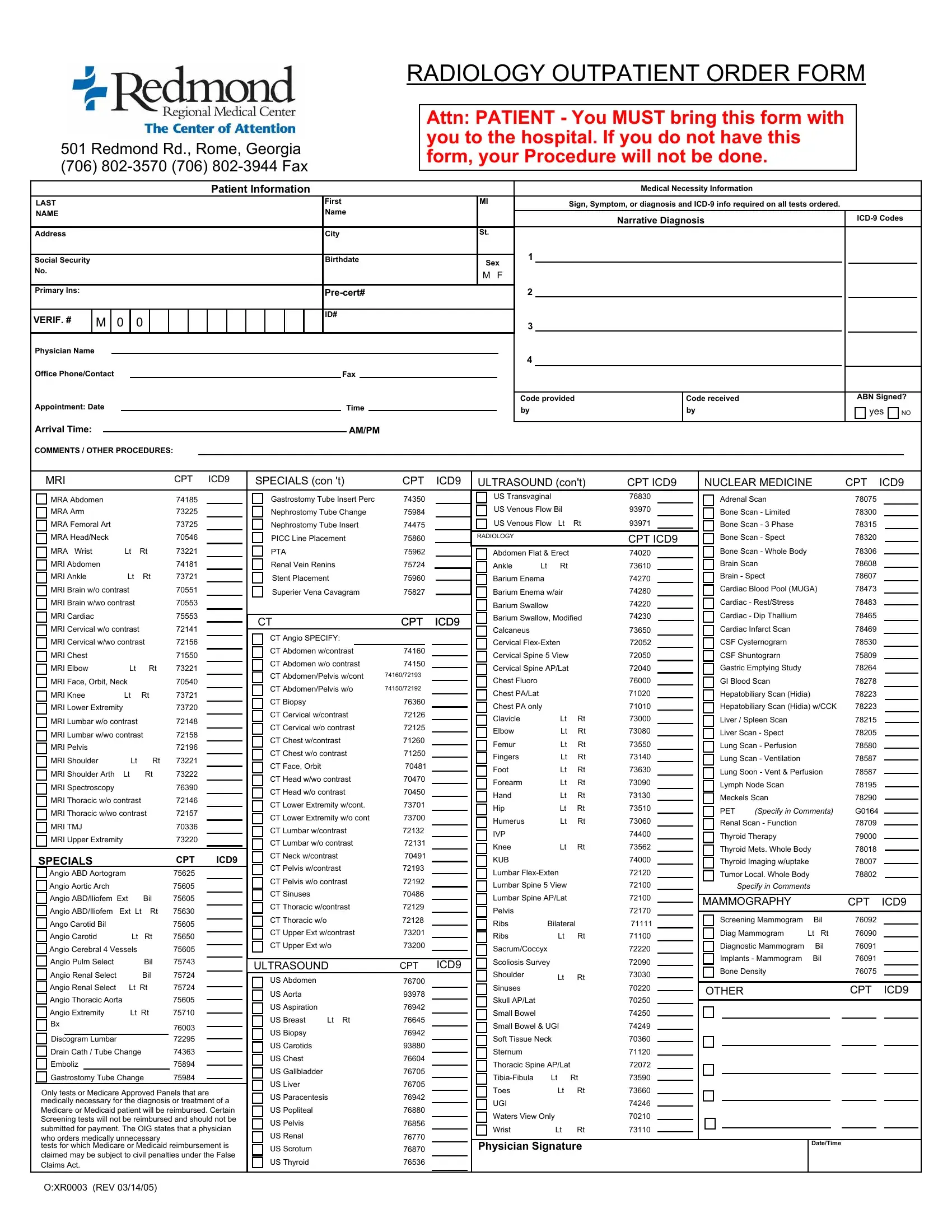
In the fast-paced, constantly evolving world of healthcare, the coordination and clarity of patient orders for radiology services are paramount. Nestled within the intricate framework of healthcare documentation, the Generic Radiology Order Form stands as a beacon of efficiency and standardization. Located at 501 Redmond Rd., Rome, Georgia, the form encapsulates crucial information, including patient details, medical necessity trivia, diagnostic codes, and an exhaustive list of possible radiologic exams and procedures, ranging from Magnetic Resonance Imaging (MRI) to Computed Tomography (CT) scans, Ultrasound evaluations, and even specialized Nuclear Medicine tests. It meticulously specifies the requisite details—such as the patient's name, address, physician's contact, and insurance verification numbers—while emphasizing the importance of the form's presence at the time of hospital arrival to facilitate the procedure. The form also serves as a guideline for medical professionals to ensure that only medically necessary and Medicare-approved tests are ordered, thereby striving to avoid unnecessary medical expenses and promote efficient patient care. This document is vital for streamlining radiology orders, ensuring accurate billing, and most importantly, enhancing patient care through precise and timely diagnostic testing.
| Question | Answer |
|---|---|
| Form Name | Generic Radiology Order Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | radiology order form pdf, mri request form, outpatient radiology order form, mri order form template |
501 Redmond Rd., Rome, Georgia
(706)
RADIOLOGY OUTPATIENT ORDER FORM
Attn: PATIENT - You MUST bring this form with you to the hospital. If you do not have this form, your Procedure will not be done.
|
|
|
|
|
|
|
|
|
|
|
Patient Information |
|
|
|
|
|
|
|
|
|
Medical Necessity Information |
|
|
|
|
|
||||||
LAST |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
First |
MI |
|
Sign, Symptom, or diagnosis and |
|
|
|
|
|
||||||||
NAME |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name |
|
|
|
|
Narrative Diagnosis |
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
St. |
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 |
|
|
|
|
|
|
|
|
Social Security |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Birthdate |
Sex |
|
|
|
|
|
|
|
|
|||||||
No. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M F |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Primary Ins: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
VERIF. # |
|
M |
|
0 |
0 |
|
|
|
|
|
|
|
|
|
ID# |
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Physician Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Office Phone/Contact |
|
|
|
|
|
|
|
|
|
|
|
|
|
Fax |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Code provided |
|
Code received |
|
|
ABN Signed? |
|||
Appointment: Date |
|
|
|
|
|
|
|
|
|
|
|
|
|
Time |
|
|
|
by |
|
by |
|
|
yes |
NO |
||||||||
Arrival Time: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
AM/PM |
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
COMMENTS / OTHER PROCEDURES:
|
MRI |
|
|
CPT |
ICD9 |
|
|
SPECIALS (con 't) |
CPT |
ICD9 |
|||||||
|
|
MRA Abdomen |
|
|
74185 |
|
|
|
|
Gastrostomy Tube Insert Perc |
74350 |
|
|
||||
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
MRA Arm |
|
|
73225 |
|
|
|
|
Nephrostomy Tube Change |
75984 |
|
|
||||
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
MRA Femoral Art |
|
|
73725 |
|
|
|
|
Nephrostomy Tube Insert |
74475 |
|
|
||||
|
|
MRA Head/Neck |
|
|
70546 |
|
|
|
|
PICC Line Placement |
75860 |
|
|
||||
|
|
MRA Wrist |
Lt |
Rt |
73221 |
|
|
|
|
PTA |
|
|
75962 |
|
|||
|
|
MRI Abdomen |
|
|
74181 |
|
|
|
|
Renal Vein Renins |
75724 |
|
|
||||
|
|
MRI Ankle |
Lt |
Rt |
73721 |
|
|
|
|
Stent Placement |
75960 |
|
|
||||
|
|
MRI Brain w/o contrast |
|
70551 |
|
|
|
|
Superier Vena Cavagram |
75827 |
|
|
|||||
|
|
|
|
|
|
|
|
|
|||||||||
|
|
MRI Brain w/wo contrast |
|
70553 |
|
|
|
|
|
|
|
|
|
|
|||
|
|
MRI Cardiac |
|
|
75553 |
|
|
|
CT |
|
|
CPT |
ICD9 |
||||
|
|
|
|
|
|
|
|||||||||||
|
|
MRI Cervical w/o contrast |
|
72141 |
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
MRI Cervical w/wo contrast |
72156 |
|
|
|
|
CT Angio SPECIFY: |
|
|
|
|
|||||
|
|
|
|
|
|
CT Abdomen w/contrast |
74160 |
|
|
||||||||
|
|
MRI Chest |
|
|
71550 |
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
MRI Elbow |
Lt |
Rt |
73221 |
|
|
|
|
CT Abdomen w/o contrast |
74150 |
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
MRI Face, Orbit, Neck |
|
70540 |
|
|
|
|
CT Abdomen/Pelvis w/cont |
74160/72193 |
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
MRI Knee |
Lt |
Rt |
73721 |
|
|
|
|
CT Abdomen/Pelvis w/o |
74150/72192 |
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
MRI Lower Extremity |
|
73720 |
|
|
|
|
CT Biopsy |
|
|
76360 |
|
|
|||
|
|
|
|
|
|
|
CT Cervical w/contrast |
72126 |
|
|
|||||||
|
|
MRI Lumbar w/o contrast |
|
72148 |
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
CT Cervical w/o contrast |
72125 |
|
|
|||||||
|
|
MRI Lumbar w/wo contrast |
72158 |
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
CT Chest w/contrast |
71260 |
|
|
||||||||
|
|
MRI Pelvis |
|
|
72196 |
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
CT Chest w/o contrast |
71250 |
|
|||||||
|
|
MRI Shoulder |
Lt |
Rt |
73221 |
|
|
|
|
|
|||||||
|
|
|
|
|
|
CT Face, Orbit |
|
|
70481 |
|
|||||||
|
|
MRI Shoulder Arth |
Lt |
Rt |
73222 |
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
CT Head w/wo contrast |
70470 |
|
|
||||||||
|
|
MRI Spectroscopy |
|
|
76390 |
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
CT Head w/o contrast |
70450 |
|
|
||||||
|
|
MRI Thoracic w/o contrast |
72146 |
|
|
|
|
CT Lower Extremity w/cont. |
73701 |
|
|
||||||
|
|
MRI Thoracic w/wo contrast |
72157 |
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
CT Lower Extremity w/o cont |
73700 |
|
|
||||||||
|
|
MRI TMJ |
|
|
70336 |
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
CT Lumbar w/contrast |
72132 |
|
|
||||||
|
|
MRI Upper Extremity |
|
73220 |
|
|
|
|
CT Lumbar w/o contrast |
72131 |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
CT Neck w/contrast |
70491 |
|
|||
|
SPECIALS |
|
|
CPT |
ICD9 |
|
|
|
|
||||||||
|
|
|
|
|
|
CT Pelvis w/contrast |
72193 |
|
|
||||||||
|
|
Angio ABD Aortogram |
|
75625 |
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
Angio Aortic Arch |
|
|
75605 |
|
|
|
|
CT Pelvis w/o contrast |
72192 |
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
Angio ABD/lliofem |
Ext |
Bil |
75605 |
|
|
|
|
CT Sinuses |
|
|
70486 |
|
|
||
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
Angio ABD/Iliofem |
Ext Lt Rt |
75630 |
|
|
|
|
CT Thoracic w/contrast |
72129 |
|
|
|||||
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
Ango Carotid Bil |
|
|
75605 |
|
|
|
|
CT Thoracic w/o |
|
|
72128 |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
Angio Carotid |
Lt |
Rt |
75650 |
|
|
|
|
CT Upper Ext w/contrast |
73201 |
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
Angio Cerebral 4 Vessels |
|
75605 |
|
|
|
|
CT Upper Ext w/o |
73200 |
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
Angio Pulm Select |
|
Bil |
75743 |
|
|
|
ULTRASOUND |
CPT |
ICD9 |
||||||
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
Angio Renal Select |
|
Bil |
75724 |
|
|
|
|
US Abdomen |
|
|
76700 |
|
|
||
|
|
Angio Renal Select |
Lt |
Rt |
75724 |
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
US Aorta |
|
|
93978 |
|
|
||||||
|
|
Angio Thoracic Aorta |
|
75605 |
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
US Aspiration |
|
|
76942 |
|
|
|||||
|
|
Angio Extremity |
Lt |
Rt |
75710 |
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
US Breast |
Lt Rt |
76645 |
|
|
|||||||
|
|
Bx |
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
76003 |
|
|
|
|
US Biopsy |
|
|
76942 |
|
|
|
|
Discogram Lumbar |
|
|
72295 |
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
US Carotids |
|
|
93880 |
|
|
||||
|
|
Drain Cath / Tube Change |
74363 |
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
US Chest |
|
|
76604 |
|
|
||||||
|
|
Emboliz |
|
|
|
75894 |
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
US Gallbladder |
|
|
76705 |
|
|
||||
|
|
Gastrostomy Tube Change |
75984 |
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
US Liver |
|
|
76705 |
|
|
||||||
|
Only tests or Medicare Approved Panels that are |
|
|
|
|
|
|
|
|||||||||
|
|
|
|
US Paracentesis |
76942 |
|
|
||||||||||
|
medically necessary for the diagnosis or treatment of a |
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
||||||||
|
Medicare or Medicaid patient will be reimbursed. Certain |
|
|
|
US Popliteal |
|
|
76880 |
|
|
|||||||
|
Screening tests will not be reimbursed and should not be |
|
|
|
US Pelvis |
|
|
76856 |
|
|
|||||||
|
submitted for payment. The OIG states that a physician |
|
|
|
|
|
|
|
|||||||||
|
|
|
|
US Renal |
|
|
76770 |
|
|
||||||||
|
who orders medically unnecessary |
|
|
|
|
|
|
|
|
|
|||||||
ULTRASOUND (con't) |
CPT ICD9 |
|||||
|
US Transvaginal |
|
76830 |
|
||
|
|
|
||||
|
US Venous Flow Bil |
|
93970 |
|
||
|
|
|
||||
|
US Venous Flow Lt |
Rt |
93971 |
|
||
|
|
|||||
RADIOLOGY |
|
|
|
CPT ICD9 |
||
|
|
|
|
|
||
|
Abdomen Flat & Erect |
|
74020 |
|
||
|
|
|
||||
|
Ankle |
Lt |
Rt |
|
73610 |
|
|
|
|
||||
|
Barium Enema |
|
|
74270 |
|
|
|
|
|
|
|||
|
|
|
|
|||
|
Barium Enema w/air |
|
74280 |
|
||
|
|
|
||||
|
|
|
||||
|
Barium Swallow |
|
74220 |
|
||
|
|
|
||||
|
Barium Swallow, Modified |
74230 |
|
|||
|
|
|||||
|
Calcaneus |
|
|
|
73650 |
|
|
|
|
|
|
||
|
|
|
|
|
||
|
Cervical |
|
72052 |
|
||
|
|
|
||||
|
Cervical Spine 5 View |
|
72050 |
|
||
|
|
|
||||
|
Cervical Spine AP/Lat |
|
72040 |
|
||
|
|
|
||||
|
Chest Fluoro |
|
|
|
76000 |
|
|
|
|
|
|
||
|
Chest PA/Lat |
|
|
|
71020 |
|
|
|
|
|
|
||
|
|
|
|
|
||
|
Chest PA only |
|
|
71010 |
|
|
|
|
|
|
|||
|
|
|
|
|||
|
Clavicle |
|
Lt |
Rt |
73000 |
|
|
|
|
||||
|
|
|
||||
|
Elbow |
|
Lt |
Rt |
73080 |
|
|
Femur |
|
Lt |
Rt |
73550 |
|
|
|
|
||||
|
|
|
||||
|
Fingers |
|
Lt |
Rt |
73140 |
|
|
|
|
||||
|
Foot |
|
Lt |
Rt |
73630 |
|
|
|
|
||||
|
Forearm |
|
Lt |
Rt |
73090 |
|
|
|
|
||||
|
Hand |
|
Lt |
Rt |
73130 |
|
|
|
|
||||
|
Hip |
|
Lt |
Rt |
73510 |
|
|
|
|
||||
|
Humerus |
|
Lt |
Rt |
73060 |
|
|
|
|
||||
|
IVP |
|
|
|
74400 |
|
|
|
|
|
|
||
|
Knee |
|
Lt |
Rt |
73562 |
|
|
|
|
||||
|
KUB |
|
|
|
74000 |
|
|
|
|
|
|
||
|
|
|
|
|
||
|
Lumbar |
|
72120 |
|
||
|
|
|
||||
|
Lumbar Spine 5 View |
|
72100 |
|
||
|
|
|
||||
|
Lumbar Spine AP/Lat |
|
72100 |
|
||
|
|
|
||||
|
|
|
||||
|
Pelvis |
|
|
|
72170 |
|
|
|
|
|
|
||
|
|
|
|
|
||
|
Ribs |
|
Bilateral |
71111 |
|
|
|
|
|
||||
|
|
|
||||
|
Ribs |
|
Lt |
Rt |
71100 |
|
|
|
|
||||
|
|
|
||||
|
Sacrum/Coccyx |
|
|
72220 |
|
|
|
|
|
|
|||
|
Scoliosis Survey |
|
72090 |
|
||
|
|
|
||||
|
Shoulder |
|
Lt |
Rt |
73030 |
|
|
|
|
||||
|
Sinuses |
|
70220 |
|
||
|
|
|
|
|
||
|
|
|
|
|
||
|
Skull AP/Lat |
|
|
|
70250 |
|
|
|
|
|
|
||
|
|
|
|
|
||
|
Small Bowel |
|
|
|
74250 |
|
|
|
|
|
|
||
|
Small Bowel & UGI |
|
74249 |
|
||
|
|
|
||||
|
Soft Tissue Neck |
|
70360 |
|
||
|
|
|
||||
|
Sternum |
|
|
|
71120 |
|
|
|
|
|
|
||
|
Thoracic Spine AP/Lat |
|
72072 |
|
||
|
|
|
||||
|
|
|
||||
|
|
Lt |
Rt |
73590 |
|
|
|
|
|
||||
|
Toes |
|
Lt |
Rt |
73660 |
|
|
|
|
||||
|
UGI |
|
|
|
74246 |
|
|
|
|
|
|
||
|
Waters View Only |
|
70210 |
|
||
|
|
|
||||
|
Wrist |
|
Lt |
Rt |
73110 |
|
|
|
|
||||
NUCLEAR MEDICINE |
CPT |
ICD9 |
|||||||
Adrenal Scan |
|
|
78075 |
|
|
|
|||
Bone Scan - Limited |
|
|
78300 |
|
|
|
|||
Bone Scan - 3 Phase |
|
|
78315 |
|
|
|
|||
Bone Scan - Spect |
|
|
78320 |
|
|
|
|||
Bone Scan - Whole Body |
|
|
78306 |
|
|
|
|||
|
|
|
|
|
|||||
Brain Scan |
|
|
78608 |
|
|
|
|||
Brain - Spect |
|
|
78607 |
|
|
|
|||
Cardiac Blood Pool (MUGA) |
78473 |
|
|
|
|||||
Cardiac - Rest/Stress |
|
|
78483 |
|
|
|
|||
Cardiac - Dip Thallium |
|
|
78465 |
|
|
|
|||
Cardiac Infarct Scan |
|
|
78469 |
|
|
|
|||
CSF Cysternograrn |
|
|
78530 |
|
|
|
|||
CSF Shuntograrn |
|
|
75809 |
|
|
|
|||
Gastric Emptying Study |
|
|
78264 |
|
|
|
|||
GI Blood Scan |
|
|
78278 |
|
|
|
|||
Hepatobiliary Scan (Hidia) |
78223 |
|
|
|
|||||
Hepatobiliary Scan (Hidia) w/CCK |
78223 |
|
|
|
|||||
Liver / Spleen Scan |
|
|
78215 |
|
|
|
|||
Liver Scan - Spect |
|
|
78205 |
|
|
|
|||
Lung Scan - Perfusion |
|
|
78580 |
|
|
|
|||
Lung Scan - Ventilation |
|
|
78587 |
|
|
|
|||
|
|
|
|
|
|||||
Lung Soon - Vent & Perfusion |
78587 |
|
|
|
|||||
Lymph Node Scan |
|
|
78195 |
|
|
|
|||
Meckels Scan |
|
|
78290 |
|
|
|
|||
|
|
|
|
|
|||||
PET |
(Specify in Comments) |
G0164 |
|
|
|
||||
Renal Scan - Function |
|
|
78709 |
|
|
|
|||
Thyroid Therapy |
|
|
79000 |
|
|
|
|||
Thyroid Mets. Whole Body |
78018 |
|
|
|
|||||
|
|
|
|||||||
Thyroid Imaging w/uptake |
78007 |
|
|
|
|||||
Tumor Local. Whole Body |
78802 |
|
|
|
|||||
|
|
Specify in Comments |
|
|
|
|
|
||
|
|
|
|
|
|||||
MAMMOGRAPHY |
|
|
CPT |
ICD9 |
|||||
|
|
|
|
|
|
||||
Screening Mammogram |
Bil |
76092 |
|
|
|
||||
Diag Mammogram |
Lt Rt |
76090 |
|
|
|
||||
Diagnostic Mammogram |
Bil |
76091 |
|
|
|
||||
Implants - Mammogram |
Bil |
76091 |
|
|
|
||||
Bone Density |
|
|
76075 |
|
|
|
|||
|
|
|
|
|
|||||
OTHER |
|
|
CPT |
ICD9 |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
tests for which Medicare or Medicaid reimbursement is |
|
US Scrotum |
76870 |
claimed may be subject to civil penalties under the False |
|
||
|
US Thyroid |
76536 |
|
Claims Act. |
|
Physician Signature |
Date/Time |
|
O:XR0003 (REV 03/14/05)