1 Last name |
First name |
MI |
Date of birth |
_ _ / _ _ / _ _ _ _ |
|
Social Security number |
Gender: m Female m Male |
Relationship: m Spouse |
m Child m Other: |
|
|
|
|
|
|
Dependent status (if applicable): |
m Full-time student m Disabled |
If disabled, indicate reason: |
|
|
|
|
|
m Add or m Delete dependent to/from my current plan for the following products: m Medical |
m Dental |
m Basic Life |
|
|
|
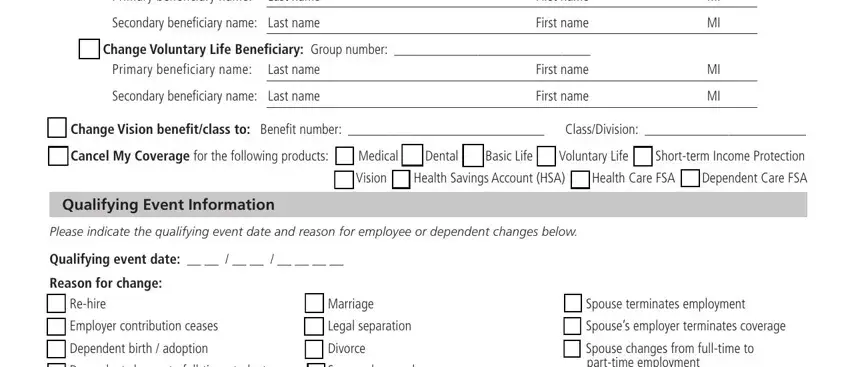
m Voluntary Life |
m Vision |
|
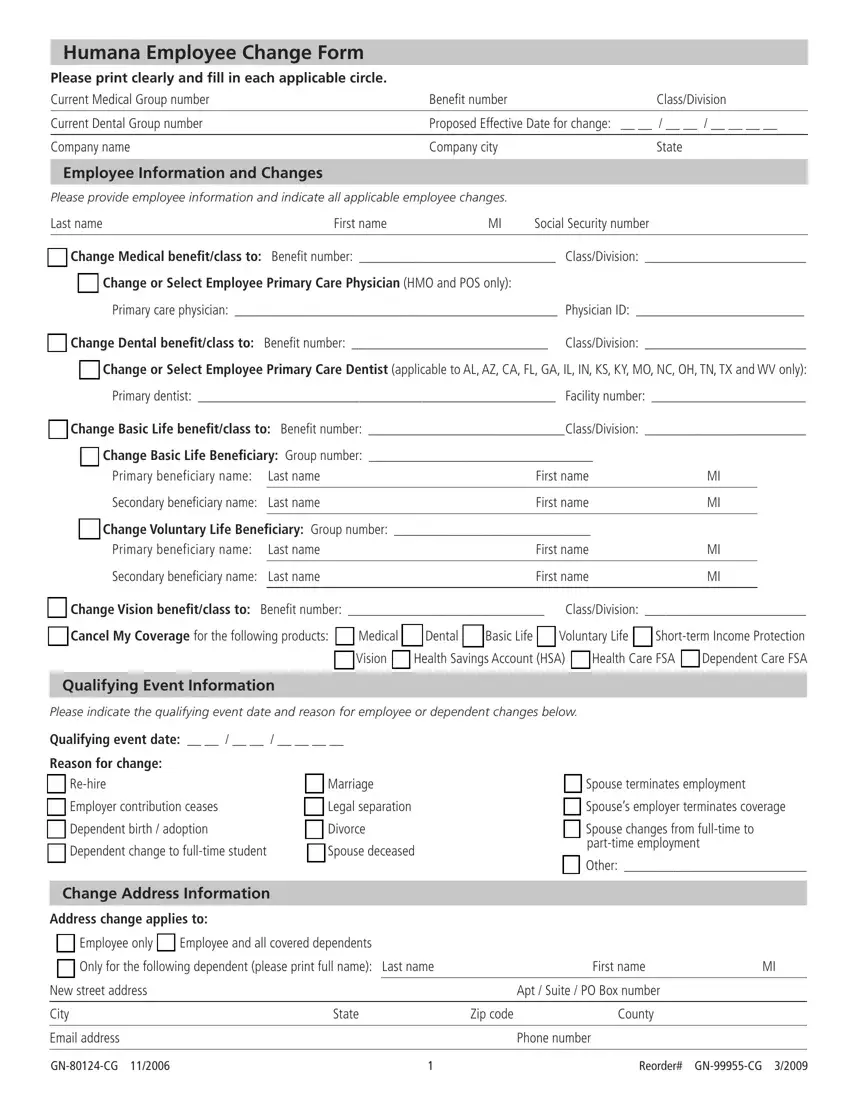
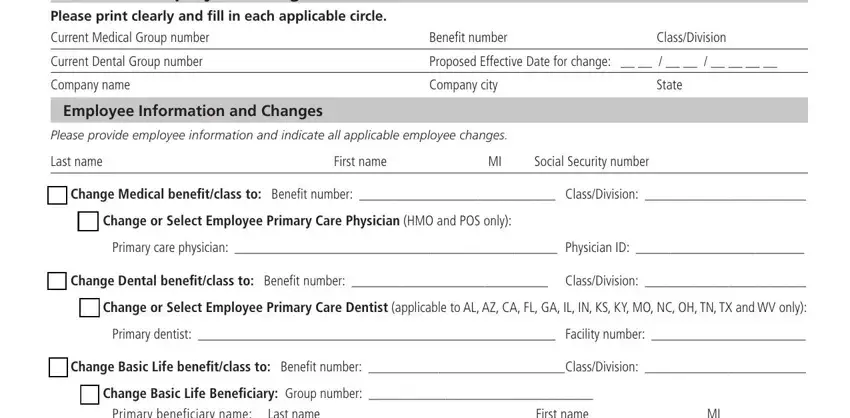
mChange or Select Primary Care Physician (HMO and POS only):
Primary care physician: __________________________________________________ Physician ID: ________________________
mChange or Select DHMO (applicable to AL, AZ, CA, FL, GA, IL, IN, KS, KY, MO, NC, OH, TN, TX and WV only):
Primary dentist: _______________________________________________________ Facility number: ______________________
|
|
|
|
|
|
|
2 Last name |
First name |
MI |
Date of birth |
_ _ / _ _ / _ _ _ _ |
|
|
Social Security number |
Gender: m Female m Male |
Relationship: m Spouse |
m Child m Other: |
|
|
|
|
|
|
|
|
Dependent status (if applicable): |
m Full-time student m Disabled |
If disabled, indicate reason: |
|
|
|
|
|
|
|
m Add or m Delete dependent to/from my current plan for the following products: m Medical |
m Dental |
m Basic Life |
|
|
|
|
m Voluntary Life |
m Vision |
|
mChange or Select Primary Care Physician (HMO and POS only):
Primary care physician: __________________________________________________ Physician ID: ________________________
mChange or Select DHMO (applicable to AL, AZ, CA, FL, GA, IL, IN, KS, KY, MO, NC, OH, TN, TX and WV only):
Primary dentist: _______________________________________________________ Facility number: ______________________
3 Last name |
First name |
MI |
Date of birth |
_ _ / _ _ / _ _ _ _ |
|
Social Security number |
Gender: m Female m Male |
Relationship: m Spouse |
m Child m Other: |
|
|
|
|
|
|
Dependent status (if applicable): |
m Full-time student m Disabled |
If disabled, indicate reason: |
|
|
|
|
|
m Add or m Delete dependent to/from my current plan for the following products: m Medical |
m Dental |
m Basic Life |
|
|
|
m Voluntary Life |
m Vision |
|
mChange or Select Primary Care Physician (HMO and POS only):
Primary care physician: __________________________________________________ Physician ID: ________________________
mChange or Select DHMO (applicable to AL, AZ, CA, FL, GA, IL, IN, KS, KY, MO, NC, OH, TN, TX and WV only):
Primary dentist: _______________________________________________________ Facility number: ______________________
4 Last name |
First name |
MI |
Date of birth |
_ _ / _ _ / _ _ _ _ |
|
Social Security number |
Gender: m Female m Male |
Relationship: m Spouse |
m Child m Other: |
|
|
|
|
|
|
Dependent status (if applicable): |
m Full-time student m Disabled |
If disabled, indicate reason: |
|
|
|
|
|
m Add or m Delete dependent to/from my current plan for the following products: m Medical |
m Dental |
m Basic Life |
|
|
|
m Voluntary Life |
m Vision |
|
mChange or Select Primary Care Physician (HMO and POS only):
Primary care physician: __________________________________________________ Physician ID: ________________________
mChange or Select DHMO (applicable to AL, AZ, CA, FL, GA, IL, IN, KS, KY, MO, NC, OH, TN, TX and WV only):
Primary dentist: _______________________________________________________ Facility number: ______________________
Signature - please sign below if requesting changes
Employee or legal representative signature: ______________________________________________ Date: ______________________
Name and relationship of legal representative: _________________________________________________________________________
GN-80124-CG 11/2006 |
2 |
Reorder# GN-99955-CG 3/2009 |