|
GSGLA PARENT PERMISSION FORM |
www.girlscoutsLA.org |
This form is REQUIRED for EVERY activity or trip, |
EMERGENCY: (877) 423-4752 |
for EACH girl, whether parents attend or not. |
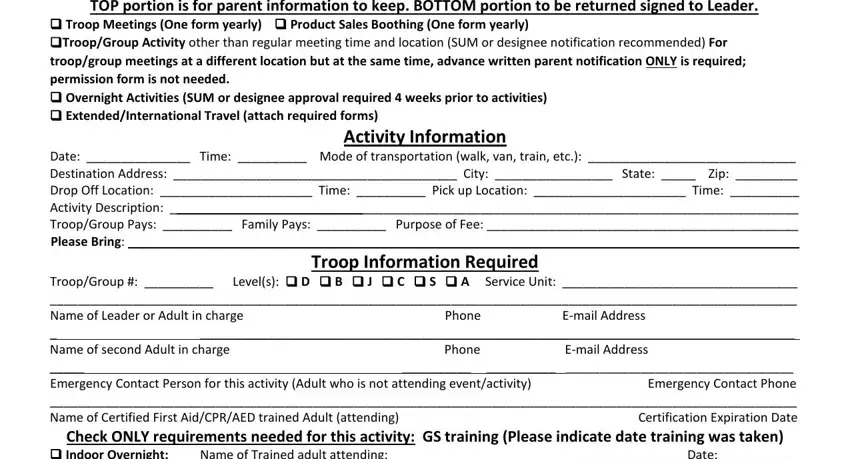
TOP portion is for parent information to keep. BOTTOM portion to be returned signed to Leader.
Troop Meetings (One form yearly) Product Sales Boothing (One form yearly)
Troop/Group Activity other than regular meeting time and location (SUM or designee notification recommended) For troop/group meetings at a different location but at the same time, advance written parent notification ONLY is required; permission form is not needed.
Overnight Activities (SUM or designee approval required 4 weeks prior to activities)
Extended/International Travel (attach required forms)
Activity Information
Date: _______________ Time: __________ Mode of transportation (walk, van, train, etc.): ______________________________
Destination Address: _________________________________________ City: _________________ State: _____ Zip: _________
Drop Off Location: ______________________ Time: __________ Pick up Location: ______________________ Time: __________
Activity Description: _ _________________________________________________________________________________________
Troop/Group Pays: __________ Family Pays: __________ Purpose of Fee: _____________________________________________
Please Bring: _________________________________________________________________________________________________
Troop Information Required
Troop/Group #: __________ Level(s): D B J C S A Service Unit: __________________________________
____________________________________________________________________________________________________________
Name of Leader or Adult in charge |
Phone |
E-mail Address |
_ |
______________________________________________________________________________________ |
Name of second Adult in charge |
Phone |
E-mail Address |
_____ |
|
__________ __________ |
_________________________________ |
Emergency Contact Person for this activity (Adult who is not attending event/activity) |
|
Emergency Contact Phone |
____________________________________________________________________________________________________________
Name of Certified First Aid/CPR/AED trained Adult (attending) |
Certification Expiration Date |
Check ONLY requirements needed for this activity: GS training (Please indicate date training was taken)
Indoor Overnight: Name of Trained adult attending: _________________________________________ Date: __________
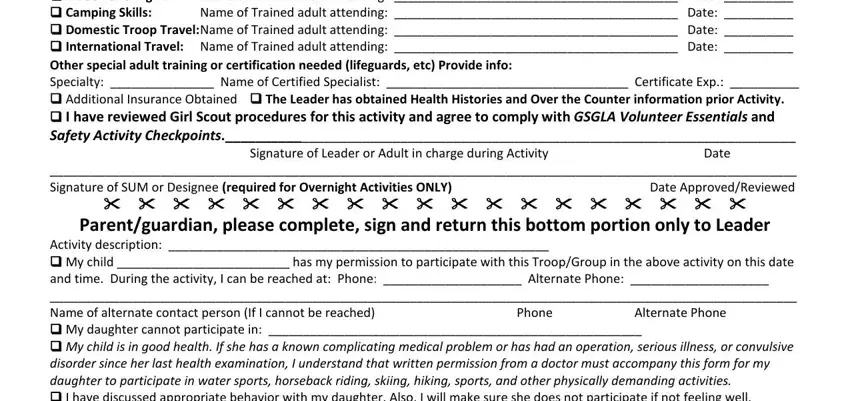
Camping Skills: Name of Trained adult attending: _________________________________________ Date: __________
Domestic Troop Travel:Name of Trained adult attending: _________________________________________ Date: __________
International Travel: Name of Trained adult attending: _________________________________________ Date: __________
Other special adult training or certification needed (lifeguards, etc) Provide info:
Specialty: _______________ Name of Certified Specialist: ___________________________________ Certificate Exp.: __________
Additional Insurance Obtained The Leader has obtained Health Histories and Over the Counter information prior Activity.
I have reviewed Girl Scout procedures for this activity and agree to comply with GSGLA Volunteer Essentials and Safety Activity Checkpoints.___________________________________________________________________________
Signature of Leader or Adult in charge during ActivityDate
____________________________________________________________________________________________________________
Signature of SUM or Designee (required for Overnight Activities ONLY)Date Approved/Reviewed
Parent/guardian, please complete, sign and return this bottom portion only to Leader
Activity description: _______________________________________________________
My child _________________________ has my permission to participate with this Troop/Group in the above activity on this date and time. During the activity, I can be reached at: Phone: ____________________ Alternate Phone: ____________________
____________________________________________________________________________________________________________
Name of alternate contact person (If I cannot be reached) |
Phone |
Alternate Phone |
My daughter cannot participate in: ______________________________________________________
My child is in good health. If she has a known complicating medical problem or has had an operation, serious illness, or convulsive disorder since her last health examination, I understand that written permission from a doctor must accompany this form for my daughter to participate in water sports, horseback riding, skiing, hiking, sports, and other physically demanding activities.
I have discussed appropriate behavior with my daughter. Also, I will make sure she does not participate if not feeling well.
___________________________________________________________________________________________ ______________
Signature of Parent/Guardian |
Date |