
You'll be able to fill in mi appraisal form effortlessly by using our online PDF tool. Our tool is consistently evolving to give the best user experience achievable, and that's thanks to our commitment to continuous development and listening closely to comments from users. Starting is effortless! Everything you need to do is take the next basic steps down below:
Step 1: Hit the orange "Get Form" button above. It will open up our pdf editor so that you could begin completing your form.
Step 2: With our state-of-the-art PDF file editor, you could accomplish more than just fill out blank form fields. Edit away and make your forms appear professional with custom textual content added in, or tweak the original input to excellence - all supported by the capability to incorporate almost any photos and sign the PDF off.
It will be easy to complete the pdf with this detailed tutorial! Here's what you should do:
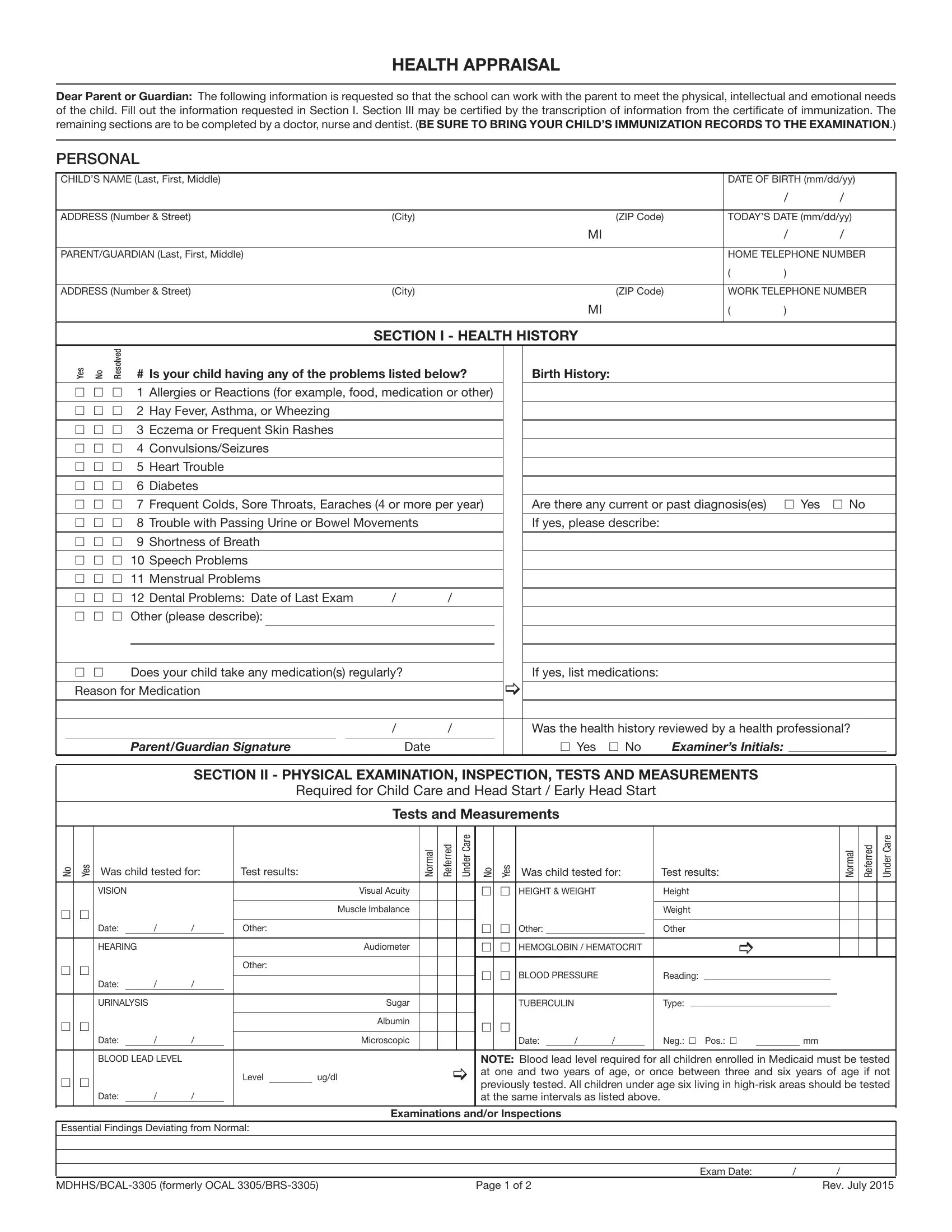
1. For starters, once filling in the mi appraisal form, start out with the section containing following blank fields:

2. Once your current task is complete, take the next step – fill out all of these fields - h h, Does your child take any, Reason for Medication, If yes list medications, ParentGuardian Signature, Date, Was the health history reviewed by, h Yes h No, Examiners Initials, SECTION II PHYSICAL EXAMINATION, Required for Child Care and Head, Tests and Measurements, o N, s e Y, and Was child tested for with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
3. Your next step is usually straightforward - fill in all of the blanks in Microscopic, Date, Neg h Pos h, Level, ugdl, NOTE Blood lead level required for, h h, Date, BLOOD LEAD LEVEL, Date, Essential Findings Deviating from, Examinations andor Inspections, MDHHSBCAL formerly OCAL BRS, Page of, and Exam Date in order to complete this part.

4. This next section requires some additional information. Ensure you complete all the necessary fields - VACCINES Circle Type, DATE ADMINISTERED, MMDDYYYY, Hepatitis B, HepB, DTaPDTPDTTd, Tdap, Haemophilus Influenzae, type b HIB, Polio, IPVOPV, Pneumococcal Conjugate, PCVPCV, Rotavirus RVRV, and MeaslesMumps Rubella MMR - to proceed further in your process!
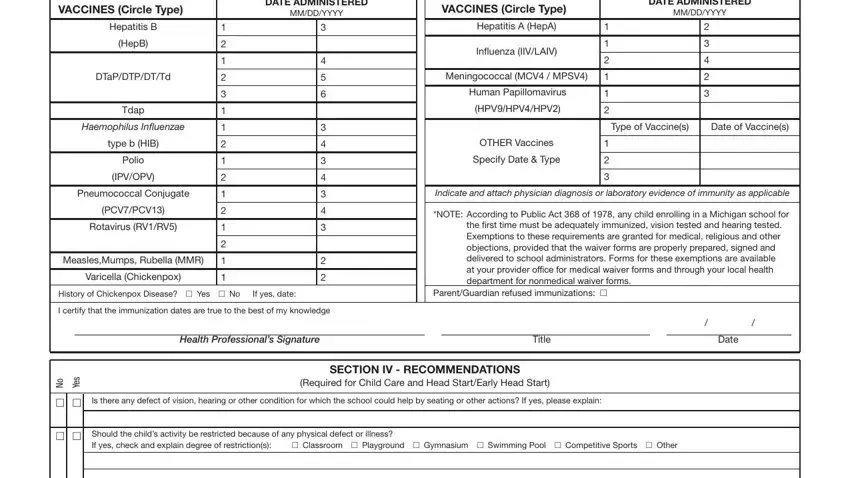
It is possible to get it wrong when completing the VACCINES Circle Type, consequently make sure to take a second look prior to deciding to finalize the form.
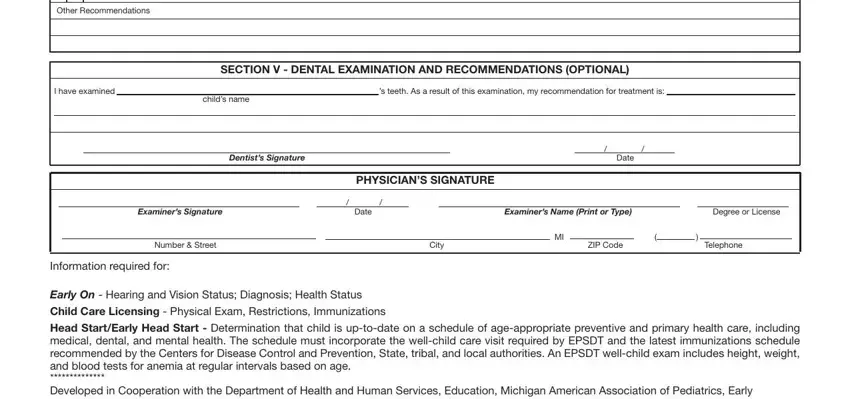
5. To finish your form, the final segment requires a number of additional fields. Entering Other Recommendations, I have examined, s teeth As a result of this, childs name, SECTION V DENTAL EXAMINATION AND, Dentists Signature, Date, PHYSICIANS SIGNATURE, Examiners Signature, Date, Examiners Name Print or Type, Degree or License, Number Street, City, and ZIP Code will conclude the process and you're going to be done very fast!
Step 3: Before finishing this form, you should make sure that form fields were filled in right. The moment you’re satisfied with it, click “Done." Go for a 7-day free trial plan at FormsPal and obtain direct access to mi appraisal form - download or modify in your FormsPal account page. Here at FormsPal, we strive to be sure that all your information is maintained protected.