
Using the online PDF tool by FormsPal, it is possible to fill out or alter humana spinal surgery orthonet form 53922 here. In order to make our tool better and simpler to utilize, we constantly develop new features, with our users' suggestions in mind. Here is what you will want to do to get going:
Step 1: Open the PDF doc inside our tool by hitting the "Get Form Button" above on this page.
Step 2: With this handy PDF editor, you are able to accomplish more than just fill out forms. Edit away and make your documents look perfect with customized textual content incorporated, or adjust the original content to excellence - all that comes along with the capability to incorporate your own graphics and sign it off.
This form requires particular info to be entered, hence be sure you take whatever time to type in exactly what is asked:
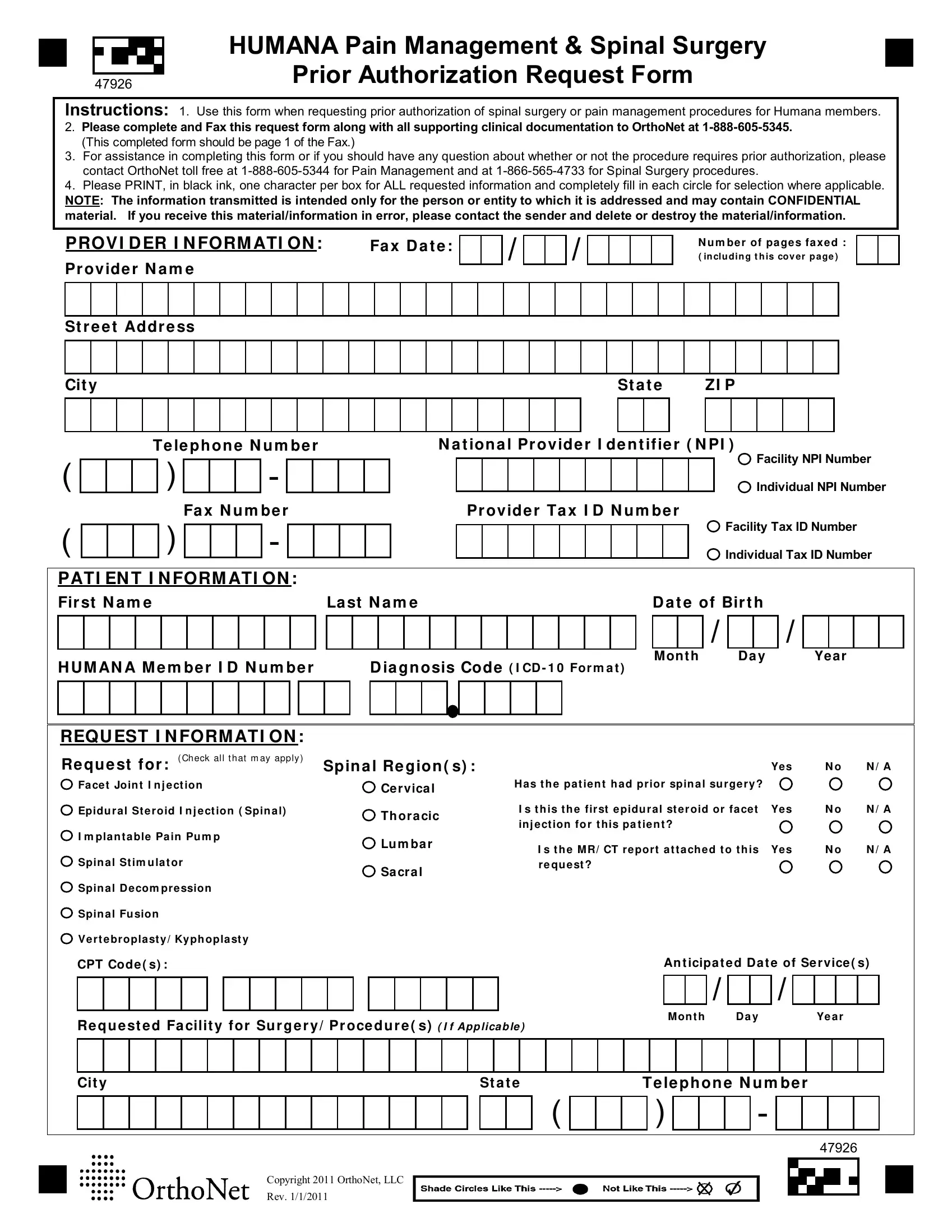
1. Fill out your humana spinal surgery orthonet form 53922 with a number of necessary blanks. Get all the necessary information and be sure nothing is omitted!
2. Once the last array of blanks is completed, go to enter the suitable information in these - REQU EST I N FORM ATI ON Check, Re qu e st f or, Fa ce t Join t I n j e ct ion, Epidu ral St eroid I n j e ct ion, I m pla n t a ble Pa in Pu m p, Spin a l St im u la t or, Spin a l D ecom pre ssion, Spin a l Fu sion, Ve rt ebropla st y Kyph opla st y, CPT Code s, Spin a l Re gion s, Yes, N o, N A, and Ce rvica l.
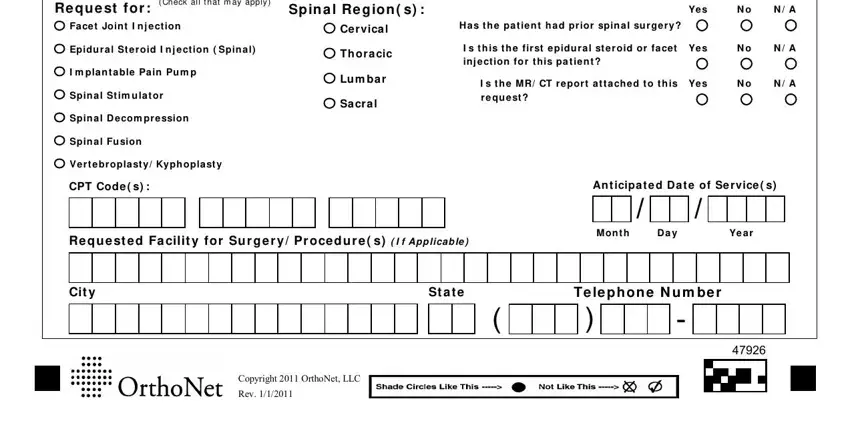
People generally make some mistakes while completing Ve rt ebropla st y Kyph opla st y in this part. Remember to revise whatever you type in here.
Step 3: Be certain that the information is right and then click on "Done" to proceed further. Right after getting a7-day free trial account at FormsPal, you will be able to download humana spinal surgery orthonet form 53922 or send it through email at once. The PDF form will also be readily available in your personal account page with your every modification. If you use FormsPal, you can certainly complete forms without being concerned about database incidents or records getting distributed. Our protected software helps to ensure that your private details are stored safe.