

You are able to fill in medical form mileage instantly with the help of our PDFinity® online PDF tool. Our professional team is constantly endeavoring to develop the editor and make it even better for users with its handy features. Unlock an ceaselessly innovative experience now - take a look at and find out new possibilities along the way! Getting underway is effortless! All you have to do is stick to these simple steps directly below:
Step 1: Access the PDF file inside our tool by pressing the "Get Form Button" at the top of this page.
Step 2: Using this state-of-the-art PDF file editor, you can actually do more than merely complete blank fields. Edit away and make your docs look high-quality with customized text incorporated, or optimize the file's original content to excellence - all that accompanied by the capability to incorporate stunning pictures and sign the PDF off.
For you to fill out this PDF document, be sure you provide the right details in every field:
1. First, while filling in the medical form mileage, start in the part that includes the next blanks:
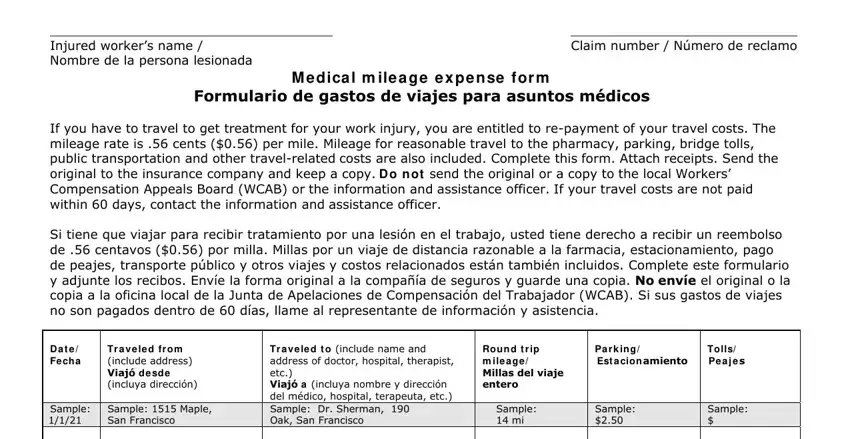
2. Once your current task is complete, take the next step – fill out all of these fields - with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
As to this field and next field, make sure you get them right here. These two could be the most important fields in this form.
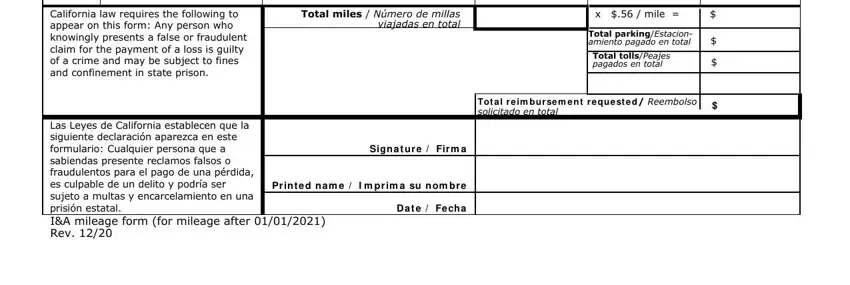
3. The following segment is normally fairly uncomplicated, California law requires the, Total miles Número de millas, x mile, Total parkingEstacion amiento, Tot a l r e im bu r se m e n t r e, Sign a t u r e Firm a, Las Leyes de California establecen, Pr in t e d n a m e I m prim a su, and D a t e Fe ch a - each one of these fields must be filled out here.
Step 3: Right after you have looked over the details in the file's blank fields, simply click "Done" to complete your form. Download the medical form mileage when you sign up for a free trial. Conveniently use the pdf file from your personal cabinet, along with any modifications and adjustments being conveniently kept! We do not share or sell any details that you enter while working with forms at our site.