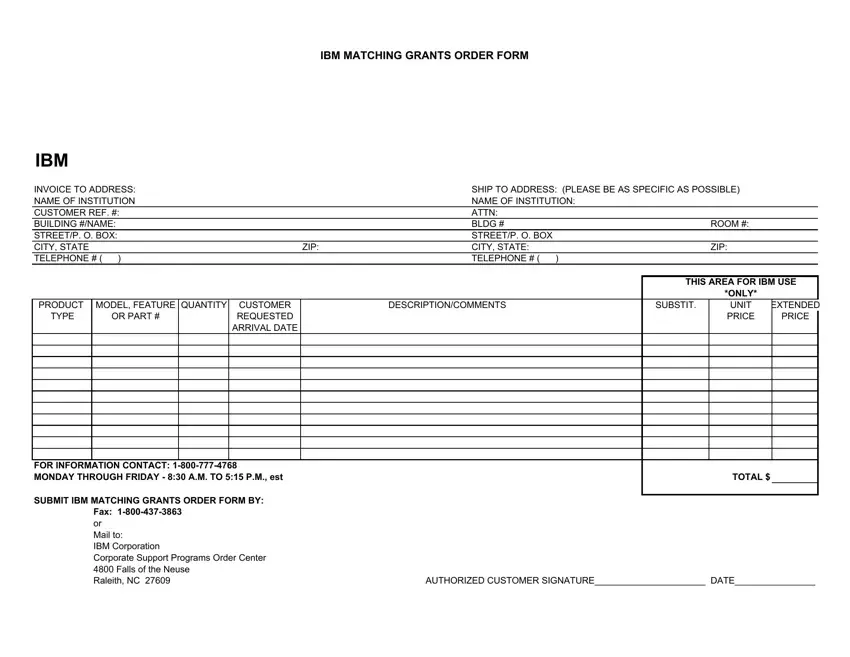
The IBM Matching Grants Program represents an invaluable opportunity for institutions seeking to maximize their technology resources through partnerships with IBM. This comprehensive program requires an official form to be filled out meticulously to ensure a successful application. The form contains several critical sections, including invoice and shipping addresses, which demand specificity for accurate processing. Identifying information such as the name of the institution, contact details, and customer reference numbers are essential to connect the request with the appropriate IBM records. Additionally, the form necessitates the detailing of product models, quantity, descriptions, and comments, allowing IBM to accurately fulfill the request or propose alternatives if necessary. The pricing and estimated arrival dates for the products are determined solely by IBM, underscoring the importance of clear and precise information from the applicant. Furthermore, the form highlights the contact information for further inquiries, submission methods via fax or mail, and mandates an authorized customer signature to validate the request. This document not only facilitates the matching grants process but also exemplifies IBM's commitment to supporting educational and institutional technology advancement.
| Question | Answer |
|---|---|
| Form Name | Ibm Matching Grants Program |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | ibm grants, mgrants us ibm com, ibm matching grants program for retirees, ibm matching grants program 2020 |
IBM MATCHING GRANTS ORDER FORM
IBM
INVOICE TO ADDRESS: |
|
|
SHIP TO ADDRESS: (PLEASE BE AS SPECIFIC AS POSSIBLE) |
|
||||||
NAME OF INSTITUTION |
|
|
NAME OF INSTITUTION: |
|
|
|||||
CUSTOMER REF. #: |
|
|
ATTN: |
|
|
|
|
|||
BUILDING #/NAME: |
|
|
BLDG # |
|
|
ROOM #: |
|
|||
STREET/P. O. BOX: |
|
|
STREET/P. O. BOX |
|
|
|
|
|||
CITY, STATE |
|
|
|
ZIP: |
CITY, STATE: |
|
|
ZIP: |
|
|
TELEPHONE # ( |
) |
|
|
|
TELEPHONE # ( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
THIS AREA FOR IBM USE |
||
|
|
|
|
|
|
|
|
|
*ONLY* |
|
PRODUCT |
MODEL, FEATURE |
QUANTITY |
CUSTOMER |
|
DESCRIPTION/COMMENTS |
|
SUBSTIT. |
UNIT |
EXTENDED |
|
TYPE |
|
OR PART # |
|
REQUESTED |
|
|
|
|
PRICE |
PRICE |
|
|
|
|
ARRIVAL DATE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FOR INFORMATION CONTACT:
SUBMIT IBM MATCHING GRANTS ORDER FORM BY: FAX:
TOTAL $
or |
|
Mail to: |
|
IBM Corporation |
|
Corporate Support Programs Order Center |
|
4800 Falls of the Neuse |
|
Raleith, NC 27609 |
AUTHORIZED CUSTOMER SIGNATURE______________________ DATE________________ |
