Seeking emergency health care can be a stressful experience, particularly when it involves navigating through complex procedures and paperwork to ensure that the care received is recognized and covered by insurance or health services. The Iowa 470 4299 form, developed by the Iowa Department of Human Services, plays a crucial role in this process for residents of Iowa. This form serves as a verification document for emergency health care services, requiring detailed information from the patient (or their guardian if the patient is a minor) such as their name, Social Security Number, date of birth, and specific details about the emergency medical condition that warranted immediate attention. It explicitly asks whether the condition was of sudden onset, leading to severe implications if not promptly treated, including severe pain, jeopardy to the patient's health, impairment of bodily functions, or serious dysfunction of any bodily part or organ. The form also inquires about labor and delivery services and whether the patient had been previously treated for a related condition. With spaces provided for detailed descriptions of the emergency condition, treatment dates, and the medical provider's information, this document is instrumental in facilitating communication between patients, healthcare providers, and the Iowa Department of Human Services. It ensures that vital emergency health care services can be appropriately verified and potentially covered, easing some of the burdens on individuals during what is often a challenging time. The authorization given by signing this document allows the release of medical information to the Department of Human Services and is valid for one year, indicating the thoughtful consideration given to the patients' privacy and the need for accurate and timely information sharing.
| Question | Answer |
|---|---|
| Form Name | Iowa Form 470 4299 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | pa emergency medicaid verification letter template, Iowa, dysfunction, specify |
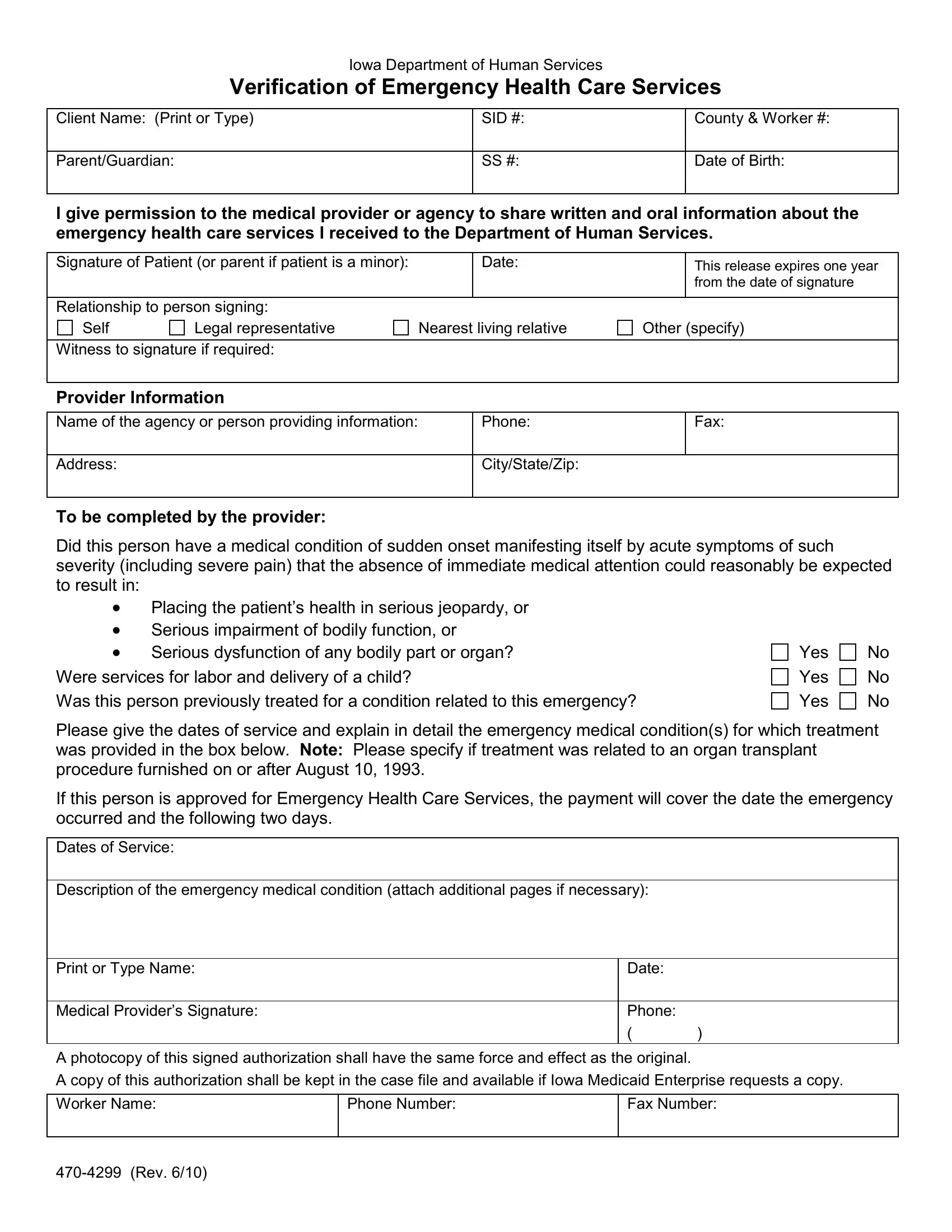
Iowa Department of Human Services
Verification of Emergency Health Care Services
Client Name: (Print or Type) |
SID #: |
County & Worker #: |
|
|
|
Parent/Guardian: |
SS #: |
Date of Birth: |
|
|
|
I give permission to the medical provider or agency to share written and oral information about the emergency health care services I received to the Department of Human Services.
Signature of Patient (or parent if patient is a minor): |
|
Date: |
|
This release expires one year |
|
|
|
|
|
|
from the date of signature |
|
|
|
|
|
|
Relationship to person signing: |
|
|
|
|
|
Self |
Legal representative |
Nearest living relative |
Other (specify) |
||
|
|
|
|
|
|
Witness to signature if required: |
|
|
|
|
|
|
|
|
|
|
|
Provider Information
Name of the agency or person providing information: |
Phone: |
Fax: |
|
|
|
Address: |
City/State/Zip: |
|
|
|
|
To be completed by the provider:
Did this person have a medical condition of sudden onset manifesting itself by acute symptoms of such severity (including severe pain) that the absence of immediate medical attention could reasonably be expected to result in:
•Placing the patient’s health in serious jeopardy, or
•Serious impairment of bodily function, or
•Serious dysfunction of any bodily part or organ? Were services for labor and delivery of a child?
Was this person previously treated for a condition related to this emergency?
Yes
Yes
Yes
No
No
No
Please give the dates of service and explain in detail the emergency medical condition(s) for which treatment was provided in the box below. Note: Please specify if treatment was related to an organ transplant procedure furnished on or after August 10, 1993.
If this person is approved for Emergency Health Care Services, the payment will cover the date the emergency occurred and the following two days.
Dates of Service:
Description of the emergency medical condition (attach additional pages if necessary):
Print or Type Name: |
Date: |
|
|
|
|
Medical Provider’s Signature: |
Phone: |
|
|
( |
) |
A photocopy of this signed authorization shall have the same force and effect as the original.
A copy of this authorization shall be kept in the case file and available if Iowa Medicaid Enterprise requests a copy.
Worker Name: |
Phone Number: |
Fax Number: |
|
|
|